
Peer Reviewed
Acute Macular Neuroretinopathy
AFFILIATION:
Geisinger Medical Center, Danville, Pennsylvania
CITATION:
Fanelli M, Tsui JC, Onishi S. Acute macular neuroretinopathy. Consultant. 2022;62(10):e18-e20. doi:10.25270/con.2022.04.00002
Received April 29, 2021. Accepted June 21, 2021. Published online July 6, 2022.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Megan Fanelli, DO, Geisinger Woodbine Lane, 16 Woodbine Lane, Danville, PA 17821 (meganelli@geisinger.edu)
A 28-year-old man initially presented to an outside eye clinic with a 6-day history of acute central blurred vision of the left eye. At that time, a central scotoma was noted on examination with a questionable macular lesion in the fundus. The patient was then referred to our urgent care eye clinic for re-evaluation 3 days later.
History. Upon presentation to our clinic, the patient reported upper respiratory symptoms, fever, and joint pain starting the day prior to the onset of visual changes (9 days prior to presentation). The patient denied associated photopsias or floaters in his vision. His medical and surgical histories were noncontributory. His ocular history consisted of myopia and contact lens use with associated contact lens–related corneal ulcers.
Physical examination. The patient had a visual acuity of 20/20 in both eyes. The pupils were equal and reactive to light, no afferent pupillary defects were noted, and normal extraocular motility and confrontational visual fields were present.
Results of a slit lamp examination did not reveal any anterior segment abnormalities, specifically no corneal changes or inflammatory cells were present to suggest uveitis. Examination of the posterior segment of the left eye revealed a well-demarcated dark spot between the fovea and optic nerve (Figure 1). No changes were observed in the right eye. The optic nerves appeared normal in both eyes.

Figure 1. Fundus photographs demonstrated a reddish-brown, wedge-shaped lesion in the nasal macula of the left eye (right) and no abnormalities in the right eye (left).
An optical coherence tomography (OCT) scan demonstrated normal thickness of the retinal nerve fiber layer bilaterally. An OCT scan of the left eye showed a hypodense area in the macula with disruption of the outer retinal layers, involving the photoreceptor layer; an OCT of the right eye showed no abnormalities (Figure 2).

Figure 2. OCT scans demonstrated disruption of the outer retina, notably the photoreceptors in the nasal macula involving the fovea in the left eye (right) and normal retina laminations of the right eye (left).
Fluorescein angiography revealed no areas of abnormalities. Humphrey Visual Field 24-2 testing revealed a small paracentral defect of the left eye and no detectable abnormalities in the right eye (Figure 3). A laboratory investigation included Epstein-Barr virus (EBV) immunoglobulin G (IgG), EBV IgM, Coxsackie A and B, streptolysin, and herpes simplex virus 1 (HSV-1) and HSV-2 IgG and IgM.
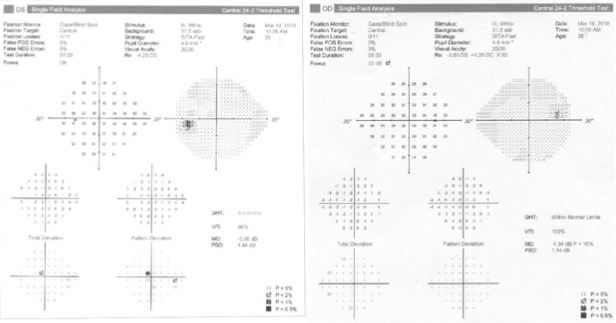
Figure 3. Humphrey Visual Field 24-2 testing demonstrated a small abnormality centrally on pattern standard deviation in the left visual field (left) and no abnormalities of the right eye (right).
On subsequent follow-up 1 week later, the patient reported no persistence of the scotoma and no development of symptoms in the right eye. Laboratory studies returned positive results for EBV IgG; all other test results were negative or were within normal limits. The patient was lost to follow-up after this visit.
Discussion. Acute macular neuroretinopathy (AMN) is a relatively rare retinal disease first described by Bos and Deutman in 1975.1 The hallmark lesion has a characteristic appearance described as a reddish-brown, wedge-shaped lesion with the apex directed toward the fovea. Patients classically present with acute-onset symptoms such as paracentral scotomas, blurred or preserved vision, and metamorphopsias.2 These visual disturbances can be transient or permanent.3 Demographically, patients presenting with AMN are more commonly women in the third decade of life and predominately of White ethnicity.2 Little is known about the pathogenesis of this disease; however, retinal ischemia due to a variety of etiologies causing disruption to the outer retinal layers is suggested as a contributing cause.4
AMN may initially present without any acute findings noted on ophthalmic examination. Absence of these characteristic lesions emphasizes the importance of imaging studies for the early detection and diagnosis of this rare disease. Near-infrared reflectance imaging and OCT are 2 important diagnostic tests used for the early detection of AMN, with identification of dark gray paracentral lesions and outer macular abnormalities, respectively.4 Visual-field testing, fluorescein angiography, and fundus autofluorescence can also aide in the diagnosis.2
A variety of macular-involved lesions have been described in the literature and have the potential to significantly impact the visual acuity of affected patients. AMN is a relatively rare retinal disorder with limited understanding of the underlying pathogenesis. Sarraf and colleagues have described an underlying vascular etiology to characterize the typical presenting lesions.4 This is due to the normal retinal anatomy whereby capillary plexuses that supply the retinal layers have varying levels of penetration, creating watershed zones. More specifically, the outer layers of the retina are highly susceptible to flow disturbances.4 Vascular etiologies that support this suggested mechanism have been described in patients with a history of shock, postpartum hypotension, and use of epinephrine. Infection and/or febrile illness and oral contraceptives have also been highly associated and described as risk factors for development of AMN.2 Classically, these patients present with acute-onset paracentral scotomas and reddish-brown, wedge-shaped paracentral lesions in the macula seen on fundoscopy.2
Delayed onset of the characteristic reddish-brown, wedge-shaped lesion can make the diagnosis of AMN difficult. Corver and colleagues describe a potential time lag between the onset of the visual deficits and the appearance of the lesions on fundoscopic examination.5 Sarraf and colleagues highlight that ophthalmoscopic abnormalities may be entirely absent with essentially normal fundus photographs on initial presentation.4 The delayed presentation of key diagnostic features can potentially be observed in our patient. Our patient initially presented to an outside eye clinic with questionable findings on fundoscopic examination and no preliminary imaging. Presentation to our urgent care eye clinic was approximately 9 days after symptom onset, and on examination, a distinct lesion was observed in his macula. A literature review revealed no definitive timeline as to when these lesions may appear in the macula.
Because identifying AMN on clinical examination can be difficult, imaging studies are of great diagnostic importance. Near-infrared reflectance imaging can demonstrate the dark-gray paracentral lesion with direction toward the fovea.4 Second, OCT scanning has shown diagnostic importance in identifying early changes in the retina.2 Bhavsar describes the combination of near-infrared imaging plus OCT as having the highest sensitivity for the diagnosis of AMN.2 Early use of these imaging tools in patients with a classic presentation for AMN may yield diagnostic results before clinical examination can detect any abnormality.2 Findings on early OCT scans include a hyperreflective layer bordering the photoreceptor layers and the outer nuclear layer with backscatter at the outer plexiform layer.6 Vaphiades observed similar findings where lesions had demonstrated focal thinning of the outer retina, potentially involving the photoreceptor outer segments with distortion of the junctions of the inner and outer segments.6
Our patient had a classic presentation for AMN. In the literature, there is a higher-reported prevalence in women, but symptom presentation regardless of gender was the most important criteria for diagnosing AMN. Our patient’s visual symptoms, preceding respiratory illness, and imaging findings all contributed to the final diagnosis. Our patient was a young man with acute-onset scotoma following the onset of upper respiratory symptoms. The hallmark reddish-brown, wedge-shaped lesion on his macula and OCT findings of disruption of outer retinal layers were present. Our patient also demonstrated a small paracentral defect in the affected eye on visual-field testing, consistent with his clinical presentation.
There has been no definitive treatment to improve or reverse retinal changes and visual symptoms. Patients can be monitored every few months, with some having improvement in visual disturbances over time, while others may have ongoing scotomas.
Conclusions. AMN is a rare retinal disease with clinical challenges to diagnosis. AMN classically presents in a typical patient population with a specific subset of presenting symptoms. Despite a limited understanding of the pathogenesis of AMN, a low threshold for imaging should be considered in patients meeting these demographic criteria and clinical presentation. Our patient demonstrated key demographic characteristics, symptoms, and clinical examination findings as noted in the literature. Initial presentation to an outside clinic demonstrated questionable macular pathology. His initial examination did not reveal the hallmark macular lesion, but our team uncovered it several days after symptom onset. Imaging modalities, specifically OCT, are of diagnostic importance in light of indeterminate clinical examination findings. As emphasized in the literature and by our patient, all patients presenting with the constellation of symptoms and demographic characteristics should undergo imaging to aid in the diagnosis of AMN.
1. Bos PJ, Deutman AF. Acute macular neuroretinopathy. Am J Ophthalmol. 1975;80(4):573-584. doi:10.1016/0002-9394(75)90387-6
2. Bhavsar KV, Lin S, Rahimy E, et al. Acute macular neuroretinopathy: A comprehensive review of the literature. Surv Ophthalmol. 2016;61(5):538-565. doi:10.1016/j.survophthal.2016.03.003
3. Özmert E, Kurt RA, Batioğlu F. Enhanced visualization of acute macular neuroretinopathy by infrared imaging and spectral optical coherence tomography. Indian J Ophthalmol. 2013;61(12):776-777. doi:10.4103/0301-4738.118461
4. Sarraf D, Rahimy E, Fawzi AA, et al. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary ischemia. JAMA Ophthalmol. 2013;131(10):1275-1287. doi:10.1001/jamaophthalmol.2013.4056
5. Corver HD, Ruys J, Kestelyn-Stevens AM, De Laey JJ, Leroy BP. Two cases of acute macular neuroretinopathy. Eye (Lond). 2007;21(9):1226-1229. doi:10.1038/sj.eye.6702543
6. Vaphiades MS, Grondines B. Occult acute macular neuroretinopathy. Neuroophthalmology. 2017;41(4):219-223. doi:10.1080/01658107.2017.1297999