
Managing Cardiometabolic Risk in CKD Patients: A Q&A With Dr James J. Matera
October 22, 2017 at 11:55am
An estimated 30 million people in the United States have chronic kidney disease (CKD), according to James J. Matera, DO, FACOI, of the Nephrology Hypertension Associates of Central New Jersey.
Furthermore, approximately 96% of people with documented CKD are unaware of this diagnosis, Dr Matera said. This lack of recognition can negatively affect outcomes in these patients, especially in regard to the risk for cardiovascular disease, which is higher among all patients with CKD.
Consultant360 recently spoke with Dr Matera, who will be presenting “Chronic Kidney Disease in Primary Care,” at the Cardiometabolic Risk Summit in Dallas, Texas.1
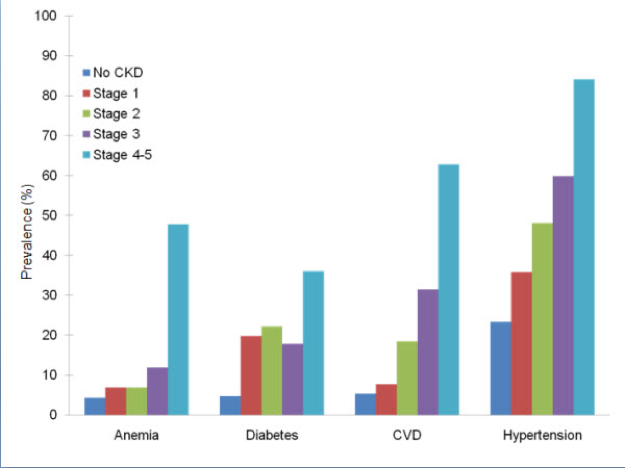
Consultant 360: How prevalent is comorbid chronic kidney disease and cardiovascular disease? How do these conditions interact?
James Matera: Having comorbid conditions with CKD predicts death. Having more comorbid conditions results in a higher hazard ratio for death. Diabetes, hypertension, cardiovascular disease, and anemia are more common in individuals who have CKD than in those who do not have CKD, and the prevalence of these comorbidities increases as CKD progresses.
C360: What screening methods exist for determining cardiovascular risk in patients with CKD?
JM: It should be recognized that CKD patients ALL have a higher risk for cardiovascular disease. They should be screened as any other patient for lipid management, reduction of risk factors, hypertension management. The impact of phosphorous on cardiovascular risk should also be recognized.
 2
2
 3
3
C360: What are the clinical implications of each category of CKD?
JM: The risks of cardiovascular morbidity and mortality increase with each stage, from stages IIIa to V. Again, having more comorbidities results in a higher hazard ratio for death.
C360: What is considered appropriate disease monitoring?
JM: I think that CKD stage III patients need to be seen every 6 months, Stage IV patients every 3 to 4 months, and Stage V who are not on dialysis every 2 to 3 months.
C360: When should a renal specialist be consulted?
JM: Great question. Some studies show earlier referrals are better, but certainly, stage IV patients should be seeing a nephrologist and beginning a relationship. This includes Care Coordination agreements and pre-ESRD [end-stage renal disease] education. This is of utmost importance, as modality choice for dialysis impacts outcomes. Use of home modalities like Home HD and peritoneal dialysis clearly improve outcomes.
—Christina Vogt
Reference:
1. Matera J. Chronic kidney disease in primary care. Presented at: Cardiometabolic Risk Summit; October 20-22, 2017. https://cardiometabolicrisksummit2017.sched.com/.
2. U.S. Renal Data System (USRDS). Chronic kidney disease in the adult NHANES population. 2009 ASRDS Annual Report Data. http://www.usrds.org/2009/pdf/V1_01_09.PDF. Accessed January 2, 2011.
3. Lesky M, Lambert A, Burden ACF, et al. The impact of chronic kidney disease and cardiovascular comorbidity on mortality in a multiethnic population: a retrospective cohort study. BMJ Open. 2013;3:e003458. doi: 10.1136/bmjopen-2013-003458.