
Peer Reviewed
Diagnostic and Treatment Challenges of Merkel Cell Carcinoma: A Case Series
Merkel cell carcinoma (MCC) is a rare neuroendocrine tumor, typically described as an asymptomatic violet, dome-shaped nodule found in a sun-exposed area. MCC is frequently misdiagnosed by clinicians, and late diagnoses can contribute to significant morbidity and mortality. We report two cases of MCC in older men with atypical presentations and highlight challenges in treatment of advanced disease.
Case 1. A 75-year-old White man presented to his dermatologist with what was previously believed to be a 2.4 cm "cyst" on his left ear (Figure 1) and associated pruitus.

Figure 1. Initial presentation of MCC in the case 1 patient, showing the "cyst" on the left ear.
History. The patient had a medical history of smoldering myeloma, hypertension, and rosacea. While not currently undergoing treatment for smoldering myeloma, the patient was prescribed losartan and metoprolol for hypertension and topical ivermectin following the use of doxycycline for rosacea.
Diagnostic testing. He underwent subsequent wide local excision (5 x 4 cm) with negative margins. A sentinel lymph node biopsy (SLNB) confirmed a diagnosis of MCC, with no evidence of nodal spread of disease. A computed tomography (CT) arterial portography and chest CT scan showed no evidence of metastasis.
Differential diagnosis. The differential diagnosis in this case included epidermal inclusion cyst and idiopathic cystic chondromalacia. The lesion was initially thought to be an epidermal inclusion cyst due to the well-circumscribed and smooth presentation. However, this diagnosis was ruled out by the pathology results. Idiopathic cystic chondromalacia are often round tumors on the ear, but are more commonly found in the upper half of the ear along the auricular cartilage rather than on the ear lobe. Pathologic diagnosis also ruled out idiopathic cystic chondromalacia.
Treatment and management. Due to the tumor size, radiation therapy of 54 gy in 22 fractions was started 3 months after diagnosis and was well-tolerated.
Outcome and follow-up. Ongoing surveillance through head and neck, chest, and abdomen and pelvis CT scans were completed at 3 month intervals from diagnosis and through 18 months of treatment. The imaging has not shown any disease recurrence.
Case 2. An 89-year-old White man presented to his dermatologist with a tender, enlarging, 8 mm subcutaneous papule with central punctum on the vertex of the scalp (Figure 2).

Figure 2. Initial presentation of MCC in case 2 patient, showing the subcutaneous papule with central punctum on the vertex of the scalp.
History. The patient had a medical history of squamous cell carcinoma of the ear, diabetes mellitus, atrial fibrillation, and severe aortic stenosis. His lesion had been present for an unknown length of time, and was being monitored by the patient and his primary care physician. However, the patient’s barber noted that it was enlarging and recommended medical evaluation.
Diagnostic testing. A shave biopsy confirmed the diagnosis of MCC. Due to the patient's age and comorbidities, resection of the primary tumor was performed with observation of lymph node basins rather than SLNB.
Differential diagnosis. The differential diagnosis for this patient included pilar or trichilemmal cyst. However, the rapid growth of the cyst would be uncharacteristic for these benign growths. The pathology results ruled out this differential diagnosis.
Treatment and management. Positron emission tomography (PET) at the time of diagnosis was suspicious for metastatic disease to the bowel and inguinal lymph nodes (Figure 3), so the patient began immunotherapy with pembrolizumab 200 mg every 3 weeks for 3 months.

Figure 3. Staging PET scan of the case 2 patient before treatment with two subcutaneous nodules along the bowel posteriorly, as well as a hypermetabolic right inguinal lymph node.
Outcome and follow-up. The patient completed four cycles of pembrolizumab, at which point a PET scan was repeated to assess response. The PET scan 5 months after diagnosis showed multiple new hypermetabolic lymph nodes in the supraclavicular, hilar, and mediastinal regions, as well as foci adjacent to the skin at the site of the primary tumor (Figure 4). Pembrolizumab was discontinued, and patient is currently undergoing immunotherapy with ipilimumab and nivolumab (ipilimumab 3 mg/kg and nivolumab 1 mg/kg every 3 weeks for 4 doses, followed by only nivolumab 480 mg intravenously every 4 weeks). Of note, 7 months after his first diagnosis, the patient developed concurrent basal cell carcinoma of the cheek, which was excised via Mohs surgery.
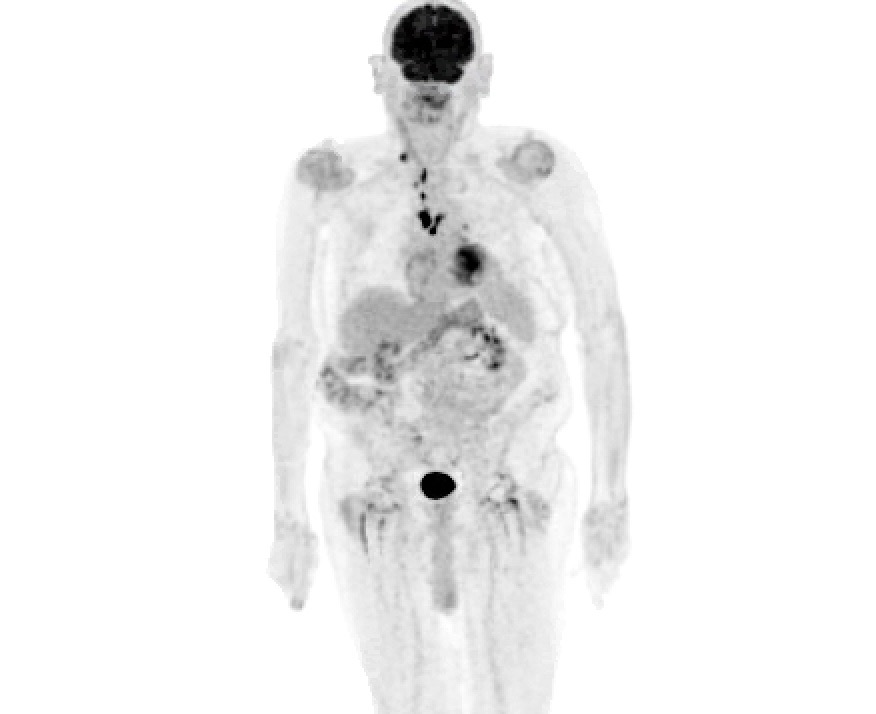
Figure 4. The PET scan of the case 2 patient following 5 months of pembrolizumab, showing multiple new hypermetabolic lymph nodes involving the right supraclavicular, mediastinal, and left hilar regions, as well as hypermetabolic foci adjacent to skin in the posterior scalp suspicious for residual disease.
Discussion. MCC is an aggressive neuroendocrine tumor with poor prognosis and high mortality rates in metastatic disease that mostly commonly presents as a rapidly growing, solitary, asymptomatic skin lesion.1 The condition is most common among older-aged men with fair-skin, especially with those who have a prolonged history of sun/ultraviolent (UV) exposure and in immunocompromised patients.2-6 More than 80% of tumors are thought to be caused by Merkel cell polyomavirus.7,8 The incidence in the United States is 0.7 per 100,000 people and is on the rise, most likely due to improved recognition of the disease and an increasing aging and immunocompromised population.9
Classic presentations of MCC are cutaneous lesions of the head and neck, described as violet, dome-shaped nodules without ulcerations found in sun-exposed areas. However, presentation varies, and lesions may appear plaque-like or as flesh-colored subcutaneous nodules, similar to benign pathologies such as cysts or lipomas, leading to frequent initial misdiagnoses.2 Rates of clinical diagnosis of MCC are low, even among dermatologists. Biopsy of seemingly benign lesions confirm the diagnosis.10 The majority of patients present with at least 3 or more of the AEIOU criteria2: asymptomatic/nontender; expanding rapidly (<3 months), immunosuppression; older than age 50 years; and location on a UV-exposed site. The wide range of presentations of MCC and relatively benign and non-specific appearance of lesions emphasizes the need for pathologic evaluation of all excised lesions, especially in high-risk populations.
Diagnosis is confirmed by histopathology and immune markers. Pathologic appearance of the tumor consists of small, round blue cells with uniform, round oval nuclei and finely dispersed chromatin.11 The majority of cases express common neuroendocrine cell markers (eg, synaptophysin, chromogranin, and neurofilament), as well as cytokeratin 20.11 The absence of melanocytic markers and TTF-1 on immunohistochemistry helps differentiate MCC from other skin cancers and to exclude cutaneous metastasis of other pathologies.12 At the time of diagnosis, 65% of patients have skin-limited disease, 26% have nodal spread, and 8% have systemic metastasis.13 Tumors may regress spontaneously or present with nodal involvement without an identifiable primary cutaneous tumor, both of which have been linked to better prognosis.14-16 Disease progression often involves spread to local lymph node basins, and common sites of organ metastasis include brain, bones, liver, and lungs.1 Staging guidelines were last updated by the American Joint Committee on Cancer in 2017. Evaluation for extracutaneous disease involves evaluation of lymph nodes, typically via physical examination and SLNB, as well as systemic evaluation via CT/magnetic resonance imaging or CT PET scan.13
Treatment varies based on the stage of disease, and consists of wide local excision, radiation therapy for regional disease, and chemotherapy for systemic metastases.17 Recently developed immunotherapies are quickly becoming the new standard of treatment for systemic disease.18 Five-year overall survival rates are approximately 50% for patients with local disease and as low as 13% for those with distant metastases.13,19
Case 1 illustrates a somewhat atypical presentation of MCC, resulting in an initial diagnosis of cyst. However, it met other AEIOU criteria; it was found in a sun-exposed area, was rapidly expanding, and present in a man aged over 50 years.2 The highly variable presentation of MCC makes recognition difficult, especially among non-dermatologist clinicians. Up to 56% of cutaneous MCC are thought to be benign at the time of biopsy, illustrating the importance of pathologic evaluation and diagnosis of what may appear to be benign lesions.11,21
Case 1 is an example of National Comprehensive Cancer Network (NCCN) Guideline–directed, multidisciplinary management of MCC, with a favorable outcome almost 1 year after diagnosis. Initial staging and management involves imaging and excision of the primary lesion, almost always followed by SLNB. Drainage basin of the primary tumor may be removed or treated with radiation when there is evidence of disease or in high-risk patients.21 Both Mohs micrographic surgery (MMS) and wide local excision have been used for excision of the primary tumor. While some evidence suggests lower rates of recurrence with MMS, retrospective comparison has not shown significant difference in overall survival.22-24 However, wide local excision remains the most common modality of excision for primary tumors and is clinically more feasible for large tumors (>T1).25 Size of the primary tumor correlates with overall survival, and adjuvant radiation for localized MCC results in improved regional control and is associated with longer disease-free survival.13,26-28 Even in cases of nodal involvement, MCC is a highly radiosensitive neoplasm; rates of recurrence after radiation are similar to those after complete lymph node dissection.29,30 Radiation may be preferred among patients who are not candidates for surgical lymph node dissection or present with large primary tumors without evidence of lymph node involvement, as seen in case 1.
Case 2 illustrates challenges in the diagnosis and management of MCC and provides an example of management beyond currently available guidelines. Per AEIOU criteria, presentation of this particular scalp lesion may also be defined as atypical given its painful, symptomatic nature and central punctum appearance, similar to an epidermoid cyst.2 Shave biopsy resulted in a pathologic diagnosis. According to current guidelines, SLNB is indicated in almost any presentation of MCC.31 However, SLNB requires the tolerance of general anesthesia and in older, sicker patients with significant comorbidities, SLNB may not be a feasible option, as seen in case 2. In these cases, staging must be done with excision and imaging alone. A baseline PET scan did not show any involvement of regional lymph nodes; however, there was hypermetabolic activity in nodules along the bowel and of an inguinal lymph node, found to be indeterminate of malignancy at the time of imaging. This imaging suggests either micrometastases of the local lymph node basin or a case of first distant metastases. While PET seems to be the imaging of choice compared with CT and has high sensitivity for detecting areas of disease, it may fail to detect micrometastases.32-35 Furthermore, studies have shown only a small proportion of patients present with metastatic disease, especially distant metastases beyond the draining lymph node basin.13,36,37 Only 13% of first metastases in MCC manifest as distant spread.38 In our patient, lack of SLNB makes it impossible to know whether micrometastases were missed in the regional lymph node basin, or if this was a true presentation of distant first metastases.
Historically, metastatic MCC was considered incurable as response to chemotherapy was often poor and short-lived.19,21 However, the advent of PD-1/PD-L1 checkpoint inhibitor therapy is becoming the standard first-line therapy for targeted treatment of metastatic disease.39 Targeted therapy such as pembrolizumab has been shown to have a better safety profile and overall survival compared with patients treated with first-line chemotherapy.40 Unfortunately, even with checkpoint inhibitor therapy, objective response rates for pembrolizumab range between 20% to 61%, as seen in this patient’s rapid progression of disease within 5 months of diagnosis after completing four cycles of pembrolizumab. Further therapeutic options for these patients are limited and involve chemotherapy, hypofractioned radiation therapy, ipilimumab, tyrosine kinase inhibitors, and intralesional treatment.41-44 For certain subsets of MCC tumors that express somatostatin receptors, somatostatin analogs may also be a mode of second-line therapy.41
Given the patient's age, tolerance, and comorbidities in this case, nivolumab, another PD-1/PD-L1 checkpoint inhibitor, and ipilimumab, an anti-CTLA-4 agent, was trialed which has shown potential synergy with PD-1/PD-L1 inhibitor therapy.42 There are few data to guide therapy for patients who do not respond to first-line therapy, especially for those who may not tolerate other second-line treatments. However, several clinical trials are underway for patients with refractory MCC to checkpoint inhibitor therapy, in the hopes that new treatment opportunities will soon be available for these patients.
Merkel cell carcinoma is a challenging but important diagnosis. Inital presenations often resemble benign conditions, and diagnosis is usually made based on pathology. We emphasize the need for sending specimens of excised lesions for pathologic evaluation, as early detection improves survival. Emerging immunotherapy offers new therapeutic options for patients, and requires the coordination of a mutlidisciplinary team to offer the best outcomes.
1. Becker JC, Stang A, DeCaprio JA, et al. Merkel cell carcinoma. Nat Rev Dis Primer. 2017;3:17077. doi:10.1038/nrdp.2017.77.
2. Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58(3):375-381. doi:10.1016/j.jaad.2007.11.020.
3. Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003;49(5):832-841. doi:10.1016/s0190-9622(03)02108-x.
4. Clarke CA, Robbins HA, Tatalovich Z, et al. Risk of Merkel cell carcinoma after solid organ transplantation. JNCI J Natl Cancer Inst. 2015;107(dju382). doi:10.1093/jnci/dju382.
5. Engels EA, Frisch M, Goedert JJ, Biggar RJ, Miller RW. Merkel cell carcinoma and HIV infection. The Lancet. 2002;359(9305):497-498. doi:10.1016/S0140-6736(02)07668-7.
6. Kaae J, Hansen AV, Biggar RJ, et al. Merkel cell carcinoma: incidence, mortality, and risk of other cancers. JNCI J Natl Cancer Inst. 2010;102(11):793-801. doi:10.1093/jnci/djq120.
7. Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science. 2008;319(5866):1096-1100. doi:10.1126/science.1152586.
8. Houben R, Shuda M, Weinkam R, et al. Merkel cell polyomavirus-infected merkel cell carcinoma cells require expression of viral T antigens. J Virol. 2010;84(14):7064-7072. doi:10.1128/JVI.02400-09.
9. Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: current United States incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78(3):457-463.e2. doi:10.1016/j.jaad.2017.10.028.
10. Burleigh A, Crawford RI. Clinical recognition of Merkel cell carcinoma by dermatologists and nondermatologists. J Cutan Med Surg. 2020;24(2):195-196. doi:10.1177/1203475419888861.
11. Pulitzer M. Merkel cell carcinoma. Surg Pathol Clin. 2017;10(2):399-408. doi:10.1016/j.path.2017.01.013.
12. Tetzlaff MT, Nagarajan P. Update on Merkel cell carcinoma. Head Neck Pathol. 2018;12(1):31-43. doi:10.1007/s12105-018-0898-2.
13. Harms KL, Healy MA, Nghiem P, et al. Analysis of prognostic factors from 9387 Merkel cell carcinoma cases forms the basis for the new 8th edition AJCC Staging System. Ann Surg Oncol. 2016;23(11):3564-3571. doi:10.1245/s10434-016-5266-4.
14. Walsh NM. Complete spontaneous regression of Merkel cell carcinoma (1986–2016): a 30 year perspective. J Cutan Pathol. 2016;43(12):1150-1154. doi:10.1111/cup.12812.
15. Foote M, Veness M, Zarate D, Poulsen M. Merkel cell carcinoma: the prognostic implications of an occult primary in stage IIIB (nodal) disease. J Am Acad Dermatol. 2012;67(3):395-399. doi:10.1016/j.jaad.2011.09.009.
16. Chen KT, Papavasiliou P, Edwards K, et al. A better prognosis for Merkel cell carcinoma of unknown primary origin. Am J Surg. 2013;206(5):752-757. doi:10.1016/j.amjsurg.2013.02.005.
17. Bichakjian CK, Olencki T, Aasi SZ, et al. Merkel cell carcinoma, version 1.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw JNCCN. 2018;16(6):742-774. doi:10.6004/jnccn.2018.0055.
18. Nagase K, Narisawa Y. Immunotherapy for Merkel cell carcinoma. Curr Treat Options Oncol. 2018;19(11):57. doi:10.1007/s11864-018-0574-5.
19. Cornejo C, Miller CJ. Merkel cell carcinoma: updates on staging and management. Dermatol Clin. 2019;37(3):269-277. doi:10.1016/j.det.2019.03.001.
20. Sihto H, Kukko H, Koljonen V, Sankila R, Böhling T, Joensuu H. Merkel cell polyomavirus infection, large T antigen, retinoblastoma protein and outcome in Merkel cell carcinoma. Clin Cancer Res Off J Am Assoc Cancer Res. 2011;17(14):4806-4813. doi:10.1158/1078-0432.CCR-10-3363.
21. Park SY, Doolittle-Amieva C, Moshiri Y, et al. How we treat Merkel cell carcinoma: within and beyond current guidelines. Future Oncol. 17(11):1363-1377. doi:10.2217/fon-2020-1036.
22. O’Connor WJ, Roenigk RK, Brodland DG. Merkel cell carcinoma. Comparison of Mohs micrographic surgery and wide excision in eighty-six patients. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 1997;23(10):929-933.
23. Gollard R, Weber R, Kosty MP, Greenway HT, Massullo V, Humberson C. Merkel cell carcinoma: review of 22 cases with surgical, pathologic, and therapeutic considerations. Cancer. 2000;88(8):1842-1851.
24. Shaikh WR, Sobanko JF, Etzkorn JR, Shin TM, Miller CJ. Utilization patterns and survival outcomes after wide local excision or Mohs micrographic surgery for Merkel cell carcinoma in the United States, 2004-2009. J Am Acad Dermatol. 2018;78(1):175-177.e3. doi:10.1016/j.jaad.2017.09.049.
25. Singh B, Qureshi MM, Truong MT, Sahni D. Demographics and outcomes of stage I and II Merkel cell carcinoma treated with Mohs micrographic surgery compared with wide local excision in the National Cancer Database. J Am Acad Dermatol. 2018;79(1):126-134.e3. doi:10.1016/j.jaad.2018.01.041.
26. Jouary T, Leyral C, Dreno B, et al. Adjuvant prophylactic regional radiotherapy versus observation in stage I Merkel cell carcinoma: a multicentric prospective randomized study. Ann Oncol. 2012;23(4):1074-1080. doi:10.1093/annonc/mdr318.
27. Bhatia S, Storer BE, Iyer JG, et al. Adjuvant radiation therapy and chemotherapy in Merkel cell carcinoma: survival analyses of 6908 cases from the National Cancer Data Base. JNCI J Natl Cancer Inst. 2016;108(9). doi:10.1093/jnci/djw042.
28. Servy A, Maubec E, Sugier PE, et al. Merkel cell carcinoma: value of sentinel lymph-node status and adjuvant radiation therapy. Ann Oncol. 2016;27(5):914-919. doi:10.1093/annonc/mdw035.
29. Leonard JH, Ramsay JR, Kearsley JH, Birrell GW. Radiation sensitivity of Merkel cell carcinoma cell lines. Int J Radiat Oncol Biol Phys. 1995;32(5):1401-1407. doi:10.1016/0360-3016(94)00610-W.
30. Sims JR, Grotz TE, Pockaj BA, et al. Sentinel lymph node biopsy in Merkel cell carcinoma: The Mayo Clinic experience of 150 patients. Surg Oncol. 2018;27(1):11-17. doi:10.1016/j.suronc.2017.10.005.
31. Xue Y, Thakuria M. Merkel cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):39-52. doi:10.1016/j.hoc.2018.08.002.
32. Colgan MB, Tarantola TI, Weaver AL, et al. The predictive value of imaging studies in evaluating regional lymph node involvement in Merkel cell carcinoma. J Am Acad Dermatol. 2012;67(6):1250-1256. doi:10.1016/j.jaad.2012.03.018.
33. Foki E, Fochtmann-Frana A, Haymerle G, et al. Computed tomography accelerates staging in patients with Merkel cell carcinoma. Eur Arch Otorhinolaryngol. 2018;275(12):3059-3066. doi:10.1007/s00405-018-5150-x.
34. Concannon R, Larcos GS, Veness M. The impact of (18)F-FDG PET-CT scanning for staging and management of Merkel cell carcinoma: results from Westmead Hospital, Sydney, Australia. J Am Acad Dermatol. 2010;62(1):76-84. doi:10.1016/j.jaad.2009.06.021.
35. Enzenhofer E, Ubl P, Czerny C, Erovic BM. Imaging in patients with merkel cell carcinoma. J Skin Cancer. 2013;2013:973123. doi:10.1155/2013/973123.
36. Kouzmina M, Koljonen V, Leikola J, Böhling T, Lantto E. Frequency and locations of systemic metastases in Merkel cell carcinoma by imaging. Acta Radiol Open. 2017;6(3). doi:10.1177/2058460117700449.
37. Edge S, Byrd DR, Compton CC, Fritz AG, Greene F, Trotti A, eds. AJCC Cancer Staging Handbook: From the AJCC Cancer Staging Manual. 7th ed. Springer-Verlag; 2010. Accessed March 28, 2021. https://www.springer.com/gp/book/9780387884424.
38. Song Y, Azari FS, Tang R, et al. Patterns of metastasis in Merkel cell carcinoma. Ann Surg Oncol. 2020;1-11. doi:10.1245/s10434-020-08587-3.
39. Pharmaceutical Approval Update. Accessed March 28, 2021. https://www-ncbi-nlm-nih-gov.proxy.lib.ohio-state.edu/pmc/articles/PMC5358679/
40. Nghiem P, Bhatia S, Lipson EJ, et al. Durable tumor regression and overall survival in patients with advanced merkel cell carcinoma receiving pembrolizumab as first-line therapy. J Clin Oncol Off J Am Soc Clin Oncol. 2019;37(9):693-702. doi:10.1200/JCO.18.01896.
41. Akaike T, Qazi J, Anderson A, et al. High somatostatin receptor expression and efficacy of somatostatin analogues in patients with metastatic Merkel cell carcinoma. Br J Dermatol. 2021;184(2):319-327. doi:10.1111/bjd.19150.
42. LoPiccolo J, Schollenberger MD, Dakhil S, et al. Rescue therapy for patients with anti-PD-1-refractory Merkel cell carcinoma: a multicenter, retrospective case series. J Immunother Cancer. 2019;7(1):170. doi:10.1186/s40425-019-0661-6.
43. Rabinowits G, Lezcano C, Catalano PJ, et al. Cabozantinib in patients with advanced Merkel cell carcinoma. The Oncologist. 2018;23(7):814-821. doi:10.1634/theoncologist.2017-0552.
44. Bhatia S, Miller NJ, Lu H, et al. Intratumoral G100, a TLR4 agonist, induces antitumor immune responses and tumor regression in patients with Merkel cell carcinoma. Clin Cancer Res Off J Am Assoc Cancer Res. 2019;25(4):1185-1195. doi:10.1158/1078-0432.CCR-18-0469.
AFFILIATIONS:
1Department of Dermatology, The Ohio State University, Columbus, OH
CITATION:
Islam N, Shipp D. Diagnostic and treatment challenges of merkel cell carcinoma: a case series. Consultant. 2023;63(10):e5. doi:10.25270/con.2023.09.000005.
Received September 27, 2022. Accepted March 10, 2023. Published online September 27, 2023.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
The authors would like to thank Carlo Contreras, Professor of Surgical Oncology at The Ohio State University, for his work in caring for these patients.
CORRESPONDENCE:
Desmond Shipp, MD, MSBS, 3a 6100 N Hamilton Road, Westerville, OH 43081 (desmond.shipp@osumc.edu)