
Managing Patients During the 2021-2022 Influenza Season
AUTHOR:
Carlos A. Arango, MD, Department of Pediatrics, University of Florida College of Medicine, Jacksonville, Florida
CITATION:
Arango CA. Managing patients during the 2021-2022 influenza season. Consultant360. Published online December 14, 2021.
Winter is coming! The temperature is dropping, and influenza is becoming more prevalent in the United States. The composition of the influenza vaccines vary every year based on the strains that are prevalent and circulating around the world at the time when health officials determine the new formulations. There are 2 types of influenza vaccines each year because the influenza season occurs at different times in each hemisphere. It tends to start in October and end in May in the northern hemisphere, and it tends to start in April and end in September in the southern hemisphere.
For the 2021-2022 influenza season, the following recommendations were made for either an egg-based vaccine or for a cell-based vaccine (Table 1). This year’s is a quadrivalent with 2 influenza A viruses and 2 different lineage of the B virus that circulated during this year’s season. For the egg-based vaccine composition, there are A/Victoria (H1N1), A/Cambodia (H3N2), B/Washington (B/Victoria lineage), and B/Phuket (B/Yamagata lineage) strains. For the cell- or recombinant-based vaccine, the only change is that one of the H1N1 strains is a Wisconsin strain.1

Data from the Centers for Disease Control and Prevention for the month of November show that there is low disease activity at this time, with only 1% of specimen results testing positive for influenza in clinical laboratories nationwide. Influenza A (H1N3) is the most prevalent, with 94% of the cases, and influenza B (Victoria lineage), with 6% of cases.2
Clinical presentation of influenza may include fever and/or chills, runny nose, sore throat, muscle or body aches, headache, and fatigue. Some gastrointestinal manifestations are more common in pediatric patients than in adults.
The only way to differentiate influenza symptoms from COVID-19, which may have a similar presentation, is to administer a nasal swab and test for both to rule out dual infection.
Influenza testing can be performed as a point-of-care in the office setting. This rapid test can be administered in the office and show results within 15 to 30 minutes. There are 2 different types of tests. One is a rapid diagnostic test, which detects antigens. The other is a rapid molecular assay, which detects the genetic material of the virus. If a more-accurate diagnostic test is desired, then a reverse transcriptase polymerase reaction can be conducted. Unfortunately, this test can only be performed at specialized laboratories, and the results may take from a few hours to a few days, depending on transport to the laboratory and turnaround time.
Rapid diagnostic tests have a moderate sensitivity (50%-70%) and high specificity. If the test has an analyzer reader, then the sensitivity increases to 75% to 80%. The rapid molecular assay has a high sensitivity of 90% to 95%. Some of these rapid tests are waived under the Clinical Laboratory Improvement Amendments of 1988 for point-of-care in the physician’s office.4
The US Food and Drug Administration (FDA) also has approved for rapid COVID-19 results to be performed as a rapid point-of-care test at your office or pharmacy and at home. Results can be obtained within 15 to 20 minutes, and like all the quick antigen tests, false-negative and false-positive test results may occur.5
Antiviral medications decrease the time of illness by only 1 to 2 days if they are prescribed early in the disease course (within 48 hours). The cost of these medications is high, even if patients have insurance coverage. Treatment tends to ameliorate the viral burden and prevent serious influenza complications, like pneumonia in high-risk groups (Table 2).
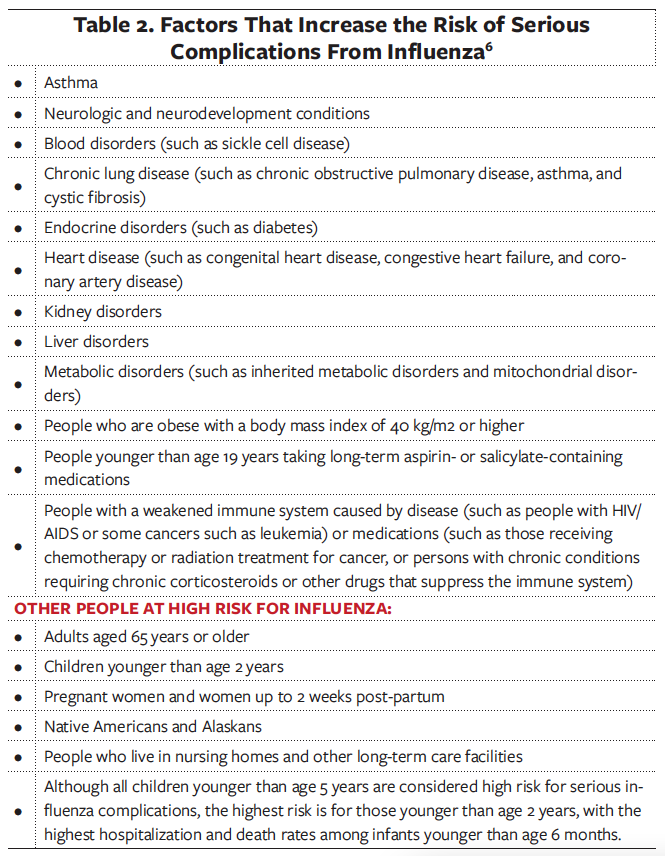
There are several treatment options for influenza infection. However, these should be prescribed only for individuals who are at high-risk—young children, people with certain medical conditions such as asthma, diabetes, and heart disease, immunocompromised patients, pregnant individuals, and adults older than age 65 years.
There are 4 FDA-approved antiviral medications available in the United States. Oseltamivir, zanamivir, peramivir, and baloxavir marboxil. Treatment is usually prescribed for 5 days orally, and peramivir is given intravenously once for people who are hospitalized.6
Due to the threat of COVID-19 and influenza this year, it is recommended that both vaccines be administered concomitantly. The Pfizer-BioNTech COVID-19 vaccine was recently approved for children aged 5 to 11 years under the FDA’s Emergency Use Authorization. Soon this population can receive this vaccine at the pediatrician’s office. This vaccine will be given as a 2-dose primary series, 21 days apart. The dose for these children is 15 µg. The dose for adolescents and adults is 30 µg. The pediatric-dose vial is orange, and the adolescent/adult dose has a purple top. If a child had received the 15-µg dose at age 11 years and is age 12 years at the time of the second dose, the child should receive the adolescent/adult dose of 30 µg for the second dose.7
Both the Pfizer and the Moderna vaccines elicited a strong immunological response against SARS-CoV-2, with a 74-fold increase in spot-forming units after vaccination. It also provided a 3-fold increase against the HCoV-NL63, a common cold coronavirus.8
We need to offer both the influenza and COVID-19 vaccines to our patients to decrease the infection rates in our part of the world.
In memorium: Jaime A. Arango. Forever in our hearts.
References:
- Frequently asked influenza (flu) questions: 2021-2022 season. Centers for Disease Control and Prevention. Reviewed November 23, 2021. Accessed November 30, 2021. https://www.cdc.gov/flu/season/faq-flu-season-2021-2022.htm#what-virus
- Weekly U.S. influenza surveillance report. Centers for Disease Control and Prevention. Reviewed November 29, 2021. Accessed November 30, 2021. https://www.cdc.gov/flu/weekly/index.htm
- Vaccines licensed for use in the United States. Centers for Disease Control and Prevention. Reviewed August 26, 2021. Accessed December 2, 2021. https://www.cdc.gov/flu/professionals/acip/2021-2022/acip-table.htm
- Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical practice guidelines by the Infectious Diseases Society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenza. Clin Infect Dis. 2019; 68(6):895-902. https://doi.org/10.1093/cid/ciy874
- COVID-19 testing overview. Centers for Disease Control and Prevention. Updated October 27, 2021. Accessed November 30, 2021. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/testing.html
- What you should know about flu antiviral drugs. Centers for Disease Control and Prevention. Reviewed August 31, 2021. Accessed November 30, 2021. https://www.cdc.gov/flu/treatment/whatyoushould.htm
- COVID-19 vaccination for children 5 through 11 years old. Centers for Disease Control and Prevention. Reviewed November 18, 2021. Accessed December 2, 2021. https://www.cdc.gov/vaccines/covid-19/planning/children.html
- Woldemeskel BA, Garliss CC, Blankson JN. SARS-CoV-2 mRNA vaccines induce broad CD4+ T cell responses that recognize SARS-CoV-2 variants and HCoV-NL63. J Clin Invest. 2021;131(10):e149335. https://doi.org/10.1172/jci149335