
Pearls of Wisdom: Smoking Cessation
A 50-year-old smoker with moderate chronic obstructive pulmonary disease (COPD) has expressed little motivation to stop smoking based on your advice and the offer of pharmacotherapy.
What additional tool might help motivate this patient to consider smoking cessation?
A. A sputum analysis
B. In-office oxygen saturation testing
C. Measurement of plasma carbon monoxide levels
D. Demonstration of lung age
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Answer: Demonstration of Lung Age
Although it is not nearly so well-recognized as the storyline of skeletal bone metabolism, wherein an ongoing osteoblast/osteoclast balance ultimately results in an age-related loss of bone mass, a similar process occurs in the lungs. The structural integrity of the lungs depends to some degree on the building and degradation of elastin, which might well be viewed as the “skeleton of the lungs.” That is, pulmonary elastase degrades elastin, while new elastin is generated through other pathways.
The enzyme responsible for signaling elastase to shut down, ending elastin degradation, is α1-antitrypsin. In persons with α1-antitrypsin deficiency, unrestrained elastase activity can lead to progressive degradation of lung tissue.
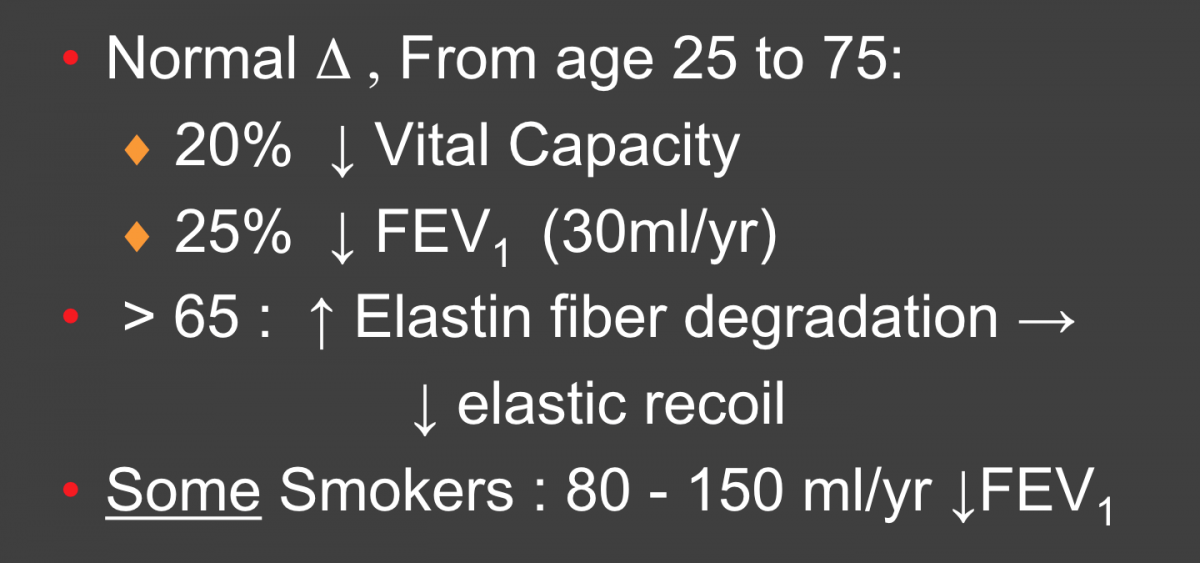
Similar to the scenario in the bony skeleton, an age-related decline in pulmonary function occurs secondary to some degree to loss of elastin, which is readily measured as a decrease in forced expiratory volume in the first second of expiration (FEV1). In otherwise healthy individuals, a loss of about 25 mL/year from young adulthood is fairly typical.1 For most healthy individuals, this degree of loss of FEV1 is insufficient to produce any meaningful pulmonary insufficiency over a lifetime.
Amazingly enough, even most smokers do not appear susceptible to the smoking-induced decrements in pulmonary function we call COPD. Only about 20% to 25% of chronic smokers develop COPD, for reasons that are ill-understood.
Concept of Lung Age2
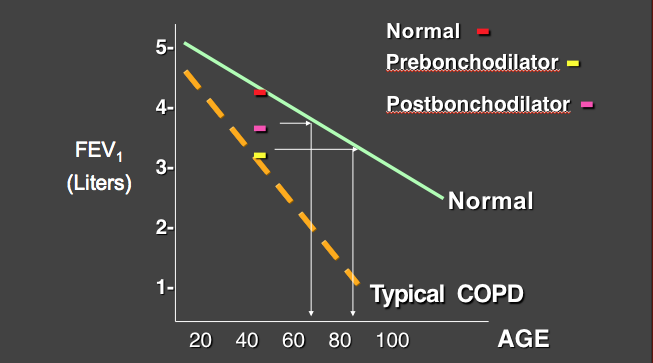
Here’s how concept of lung age can be used:
- Along the y-axis is FEV1, and along the x-axis is the patient’s age.
- The green line is the normal age-related decline in FEV1 seen in nonsmokers.
- The dotted orange line is the line of pulmonary function decline that might be seen in a typical susceptible smoker.
- The yellow dash is the result on office pulmonary function testing that our 50-year-old smoker has achieved.
Our patient has an FEV1 of about 3.2 L; that number is not atypical for smokers and, indeed, falls right on the orange line of typical decline for susceptible smokers. A line connecting that 3.2 L FEV1 (yellow) to the normal line (green) indicates that this FEV1 would be normal for an 85-year-old!
Normal FEV1 function at this age would be about 4.5 L (red dash). We can offer some hope that bronchodilators might improve FEV1 from 3.2 L to 3.5 L (pink dash), but even then, our patient would still be measured as having lung function appropriate for a 65-year-old!
Aging and the Lung1
In my experience, smokers quit for a variety of reasons. Sometimes an acute illness convinces them. Sometimes a fright from an abnormality on a chest radiograph, or learning that a friend or loved one has incurred lung cancer, is the wake-up call they need. Unless they are quite sophisticated, the reporting of simple FEV1/forced vital capacity results to patients may not impress, since they have little way to conceptualize just what a “25% decrease in FEV1” means.
Try this: Most individuals at all levels of education can interpret the gravity of having the lungs of an 85-year-old when the person is just 50 years old.
FEV1 Decline: Age and Smoking History4
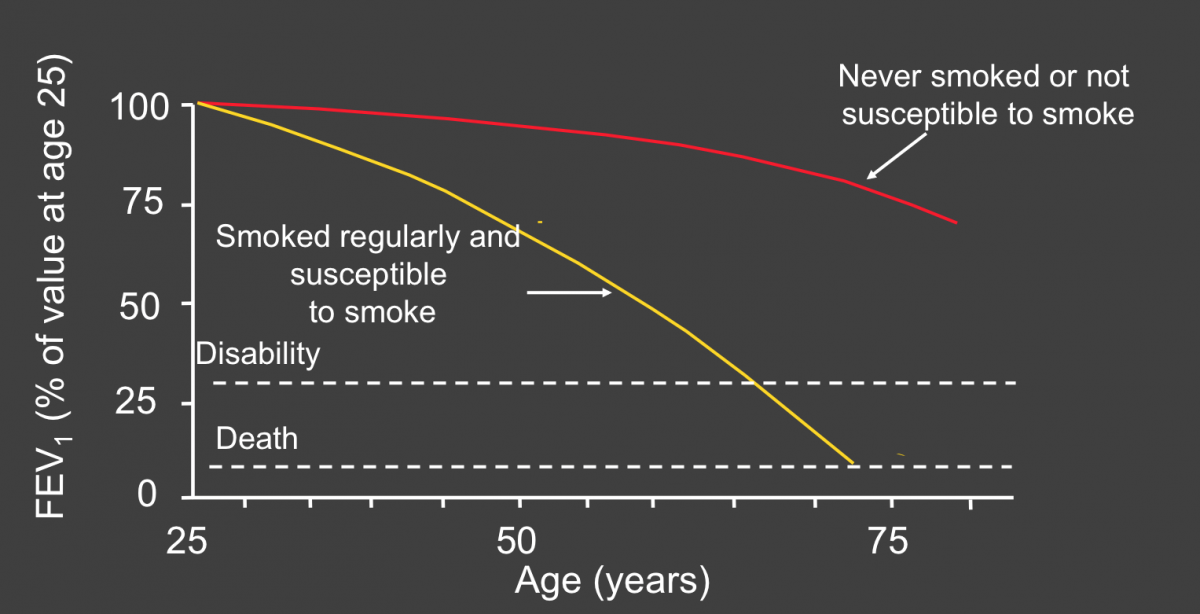
As discouraging as it might sound to be informed that one has the lungs of an 85-year-old, smokers should at the same time be informed that it’s never too late to quit. Smoking cessation at any time will blunt the decline in lung function.4
What’s the “Take Home”?
Patients quit smoking for a variety of reasons, not the least of which is a strong signal that smoking is damaging their health. The concept of lung age is a straightforward way to introduce smokers—in a readily conceptualized manner—to the magnitude of lung damage they are incurring. Additionally, a clinical trial using this tool has confirmed enhanced quit rates compared with simply informing patients of their spirometry results in the traditional fashion.3
References:
- Pulmonary problems. In: Barker LR, Burton JR, Zieve PD, eds. Principles of Ambulatory Medicine. 5th ed. Baltimore, MD: Williams & Wilkins; 1999.
- Morris JF, Temple W. Spirometric “lung age” estimation for motivating smoking cessation. Prev Med. 1985;14(5):655-662.
- Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336(7644):598-600.
- Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J. 1977;1(6077):1645-1648.