
Pearls of Wisdom: Congestive Heart Failure
Mark is a 62-year-old African American man with a 2-year history of congestive heart failure (CHF). His New York Heart Association class III CHF (ejection fraction, 35%) severely limits his daily activities. As a result, his quality of life has gone down substantially in the past year. He is unable to engage in any strenuous physical activity and becomes problematically short of breath from simply trying to climb a flight of stairs. He has even converted his downstairs den into a bedroom.
His medical history includes a 15-year history of hypertension and obesity. An echocardiogram confirmed systolic dysfunction but no correctable lesions. His kidney function is good (serum creatinine, 1.0 mg/dL), and his electrolytes were within normal limits.
He presented to the office with a blood pressure of 132/82 mm Hg, a pulse of 68 beats/min, a temperature of 37°C, and a weight of 85.3 kg (body mass index, 29 kg/m2 and stable over the past 6 months). Physical examination showed mild bibasilar rales and trace ankle edema.
His medication regimen includes losartan, 100 mg/d; metoprolol succinate, 200 mg/d; spironolactone, 25 mg/d; aspirin, 81 mg/d; and furosemide, 40 mg/d.
At rest, the patient is comfortable but unable to engage in much activity due to shortness of breath. What next step might improve Mark’s quality of life and reduce his risk of mortality?
A. Add digoxin.
B. Increase the dose of furosemide.
C. Increase the dose of spironolactone.
D. Add isosorbide dinitrate plus hydralazine.
How do you advise your patient?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Add isosorbide dinitrate plus hydralazine.
Perhaps because CHF is so common among older adults, or perhaps because we have such a diversity of pharmacologic agents to successfully treat it, the gravity of the CHF diagnosis sometimes escapes us. Indeed, for years I have called CHF the “hemodynamic malignancy.” Why? Because once the diagnosis of CHF has been made, patient outcomes are often worse than with most cancers!
Almost 20 years ago, articles in major journals1 dramatized the plight of CHF patients. We can be grateful for the inroads that we have made in CHF thanks to positive clinical trials affirming the mortality-reducing impact of angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), β-blockers, and aldosterone antagonists (ie, spironolactone and eplerenone), but there is still much room for improvement.
_______________________________________________________________________________________________________________________________________________________________________
RELATED STORIES
Pearls of Wisdom: Getting the Genie Back Into the Bottle…and Other Magic
Pearls of Wisdom: Vitamin Supplementation in Smokers
_______________________________________________________________________________________________________________________________________________________________________
The A-HeFT Trial
Comprehensive treatment of CHF requires symptomatic treatment (usually loop diuretics) and disease-modifying therapy (eg, ACEIs, ARBs, β-blockers, and aldosterone antagonists). However, the treatment that often is inadvertently left off of this menu is the combination of isosorbide dinitrate plus hydralazine, which has been proven to have a clinically meaningful and statistically significant impact on not only mortality but also quality of life.2
An earlier trial, the Vasodilator-Heart Failure Trial (V-HeFT),3 found that vasodilator therapy had a markedly favorable impact only on the African American subgroup of the trial, but not on all participants. Since this observation was the result of subgroup analysis that had not been a prespecified trial outcome, it had to be confirmed in a separate prospective trial—hence, the African-American Heart Failure Trial (A-HeFT).2
A-HeFT studied more than 1000 African Americans who were already receiving standard-of-care regimens (eg, ACEIs or ARBs, β-blockers, spironolactone). In this placebo-controlled trial, the addition of isosorbide dinitrate plus hydralazine showed dramatic, prompt, favorable outcomes.
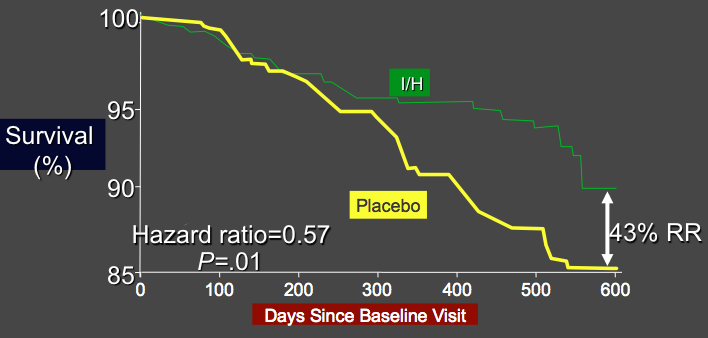
A-HeFT Composite Score Individual Components: Death2
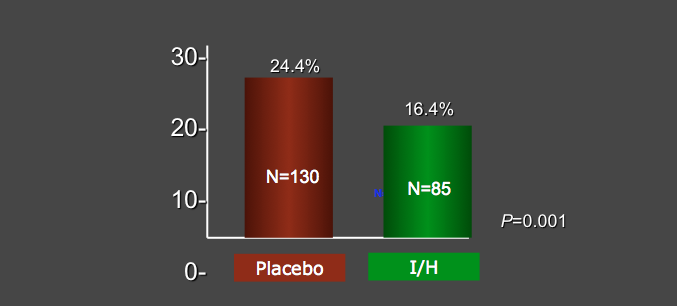
A-HeFT Composite Score Individual Components: First CHF Hospitalization2
Indeed, the trial had to be stopped early because of the favorable impact of the treatment on mortality.
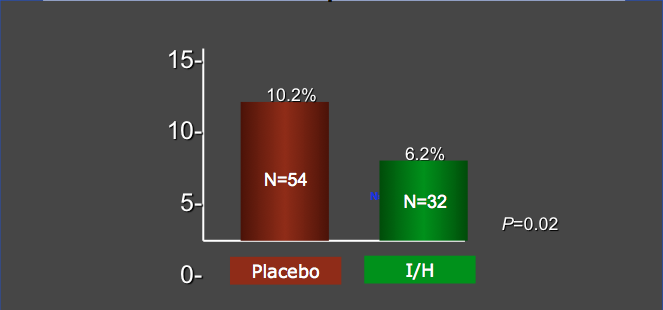
A-HeFT Composite Score Individual Components: Mortality2
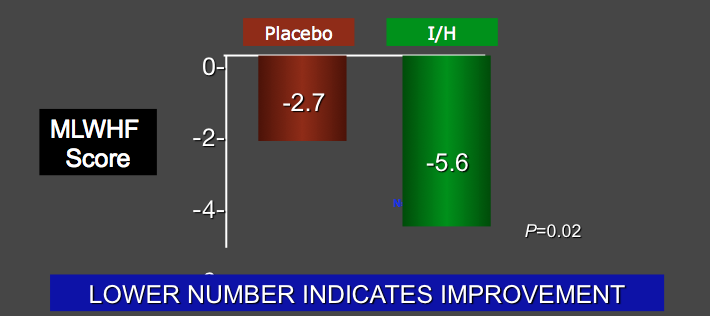
In addition to the “hard” endpoint of mortality, the Minnesota Living with Heart Failure questionnaire—a 21-item self-administered survey that queries commonplace obstacles faced by persons with CHF—was used to assess quality of life.
The favorable outcomes in A-HeFT were consistent, meaningful, and impressive, and they occurred rapidly. Overall, patients treated with isosorbide dinitrate plus hydralazine had a 42% reduction in mortality, a longer duration before being readmitted for CHF, and improved quality of life.
A-HeFT Composite Score Individual Components: Quality of Life Change2
Treatment Standards
Well, with these impressive results, why isn’t every African American person with CHF on this combination of drugs? A number of explanations have been offered.
Perhaps clinicians are not confident in determining who is African American and who is not. For example, if a patient has one African American parent and one Asian parent, is he African American or not? Technically, the question should not be that difficult, since inclusion in the trial only required that the patient self-identify as an African American—so it’s really not up to the clinician at all.
A-HeFT Conclusions2
Second, perhaps clinicians were concerned that isosorbide dinitrate plus hydralazine would be poorly tolerated or lead to troublesome adverse effects. This was not seen in the clinical trial.
Third, some clinicians were distressed that 2 pharmacologic entities that were individually generic (and hence inexpensive) at the time of the trial, when combined into a single fixed-dose combination pill, became remarkably more expensive as a proprietary new product.
Whatever the obstacle clinicians have had to use isosorbide dinitrate plus hydralazine as a component of CHF treatment, it is time to remove it. In the absence of an absolute contraindication to either of the ingredients, every African American with systolic dysfunction who is similar to the population studied in A-HeFT should be treated with isosorbide dinitrate plus hydralazine—both to reduce their mortality and to improve their quality of life.
What’s the “Take Home”?
Although much improved in the past decade, the outcomes for patients with CHF are still daunting. A therapeutic regimen for CHF in African American patients should include an ACEI or ARB, β-blocker, aldosterone antagonist, and the combination of isosorbide dinitrate plus hydralazine before being considered complete. Selection for this treatment should depend on a patient's self-designation as African American.
References:
- Mulrow CD, Mulrow JP, Linn WD, Aguilar C, Ramirez G. Relative efficacy of vasodilator therapy in chronic congestive heart failure: implications of randomized trials. JAMA. 1988;259(23):3422-3426
- Taylor AL, Ziesche S, Yancy C, et al; African-American Heart Failure Trial Investigators. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351(20):2049-2057.
- Cohn JN, Archibald DG, Ziesche S, et al. Effect of vasodilator therapy on mortality in chronic heart failure. N Engl J Med. 1986;314(24):1547-1552.