
Multigenerational Women With Migraine and Early Stroke
Authors:
Sidish S. Venkataraman, BSA; Jocelyn E. Abraham, BA; Fatima Aly, MD; and Lynnette J. Mazur, MD, MPH
Department of Pediatrics, McGovern Medical School at UTHealth, Houston, Texas
Citation:
Venkataraman SS, Abraham JE, Aly F, Mazur LJ. Multigenerational women with migraine and early stroke [published online October 5, 2018]. Neurology Consultant.
A 15-year-old girl with a history of chronic migraine presented to the clinic with what she called the worst headache of her life. She described the pain as bifrontal, throbbing, and associated with photophobia, photopsia, phonophobia, blurred vision, and perioral tingling. She denied any changes in speech or weakness in her arms or legs.
History. Her migraines had started at age 12 and were usually preceded by up to 30 minutes of photopsia, or migraines with aura (MA). They occurred 4 to 6 times per week. Diet history revealed that she regularly skipped meals and had poor sleep hygiene; she took 2- to 3-hour naps after school and slept at night from 1 am to 6 am. Her maternal family history included 4 generations of women with MA and early stroke (Figure 1).
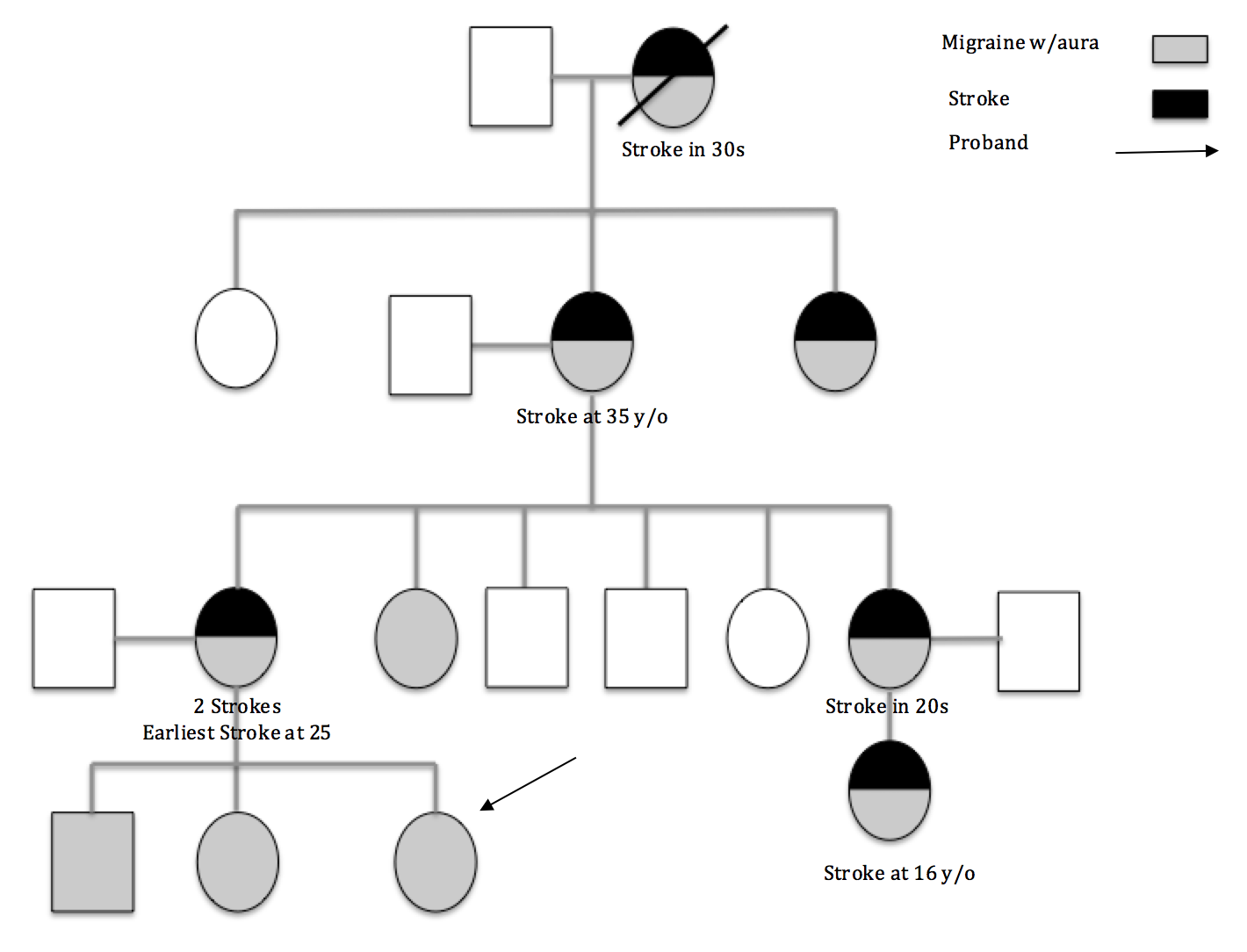
Figure 1. A pedigree outlining the patient’s family history of migraine and stroke.
Physical examination. The only pertinent physical finding was a body mass index of 35.9 kg/m2 (99th percentile). No neurologic abnormalities were noted.
Diagnostic tests. Computed tomography (CT) and CT angiography (CTA) performed in the emergency department showed no signs of hemorrhage or vascular occlusion. Later, magnetic resonance imaging showed punctate foci of T2/FLAIR (fluid-attenuated inversion recovery) hyperintense signal in the periventricular and deep white matter of the frontal lobes, which may be sequelae of migraines (Figure 2).
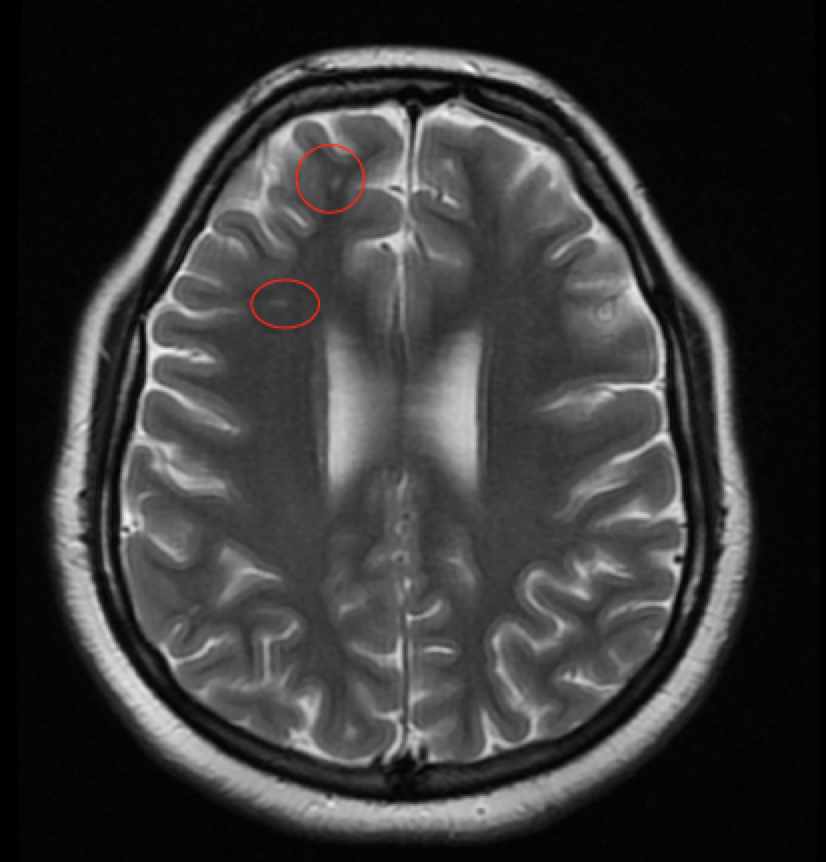
Figure 2. T2-weighted MRI of the brain taken on the day of presentation. Circled in red are two examples of the punctate hyperintense signal seen in the periventricular and deep white matter of the frontal lobes. These changes likely are sequelae of migraines.
Propranolol and vitamin D supplements were prescribed, and regular meals and a better sleep routine were recommended.
Discussion. Migraines are characterized by recurrent headaches with at least 3 of the following features: abdominal pain, nausea or vomiting, throbbing pain, unilateral location, aura (visual, sensory, or motor), relief after sleep, and a positive family history.1 Migraines without aura, previously known as common migraines, account for 60% to 80% of migraines. MA, previously known as classic migraines, have fully reversible auras that may include blurred vision, scotoma (areas of depressed vision within the visual field) photopsia (flashes of light), fortification spectra (brilliant white zig-zag lines), perceived distortion of objects, and hallucinations. Somatosensory aura, perioral paresthesias and/or numbness, and tingling of the hands and feet are less common.1,2 Chronic migraines, in contrast with episodic migraines, occur on more than 15 days per month.
The prevalence of migraines increases with age and reaches up to 10% in children. Gender distribution is equal before puberty but shifts to a 3 to 1 female preponderance after puberty.2,3 Approximately 50% of affected persons have a first-degree relative with migraines. While the etiology is poorly understood, the 2 main theories are vasodilation in the cerebral vasculature and activation of peripheral nerves, including the trigeminal ganglia, which causes modulation of sensory activity.4 Aura is thought to occur when a cortical wave of electrophysiologic hyperactivity spreads across the brain. A wave of inhibition follows, leading to ischemia, resolution of the aura, and the beginning of a headache.5
Pharmacologic treatment of acute migraines includes the use of analgesics and antiemetics. Prophylaxis is recommended for patients experiencing 4 to 6 migraines a month. Because there is an association with vitamin D deficiency, supplementation can be helpful.6 A healthy diet and good sleep hygiene are also important.7-9 Because the risk of ischemic stroke is 1.7-fold higher when using oral contraceptives, the avoidance of estrogens is advisable.10
Our patient’s extended family history of migraine and stroke suggested a causal relationship. MA increases the risk of stroke by more than 50%, but there is no increased risk with migraines without aura.11-13 Familial hemiplegic migraine, a subtype of MA, is characterized by an autosomal dominant pattern of inheritance and weakness/hemiparesis during the aura. Three genes located on 1q33, 2q24, and 19p13 increase glutamate and potassium in the synaptic cleft and increase the risk for cortical spreading depression.3
Discerning the relationship between migraine and stroke is difficult, but 4 theories have been proposed. First, migraine-induced strokes may be precipitated by cortical spreading depression. Second, the 2 may share a common underlying disorder such as cerebral autosomal arteriopathy with subcortical infarcts and leukoencephalopathy or mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes.3
Third, both migraines and transient ischemic attacks (TIAs) are associated with temporary neurological deficits. With typical symptoms, the aura of migraines progress gradually, last less than 30 minutes, and resolve with a headache; symptoms of TIAs occur suddenly, last less than 15 minutes, and resolve without a headache. However, basilar TIAs may be associated with headache, obscuring this difference. Fourth, the 2 may independently coexist (Table).3 Identification of an underlying cause may prevent recurrence, which affects up to 20% of patients.13
Table. Possible Relationship Between Migraines and Stroke |
1. Migraines precipitate stroke |
2. Migraines and stroke share a common underlying disorder |
3. Migraines mimic strokes or TIAs |
4. Migraines and stroke independently coexist |
The long-term prognosis of migrainous infarction is unclear. One study showed that 50% of patients recovered without sequelae and that migraine frequency was reduced afterwards.14 Recommendations for stroke prophylaxis are also unclear, but aspirin and other nonsteroidal medications may be effective in preventing migraines and ischemic stroke.15
Our patient and her family illustrate a strong association between MA and early stroke. When considering a diagnosis of migraine, inquire about MA and strokes in the family history. Lifestyle modifications and pharmacologic treatment are especially important in these patients.
References:
- Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629-808.
- Özge A, Termine C, Antonaci F, Natriashvili S, Guidetti V, Wöber-Bingöl Ç. Overview of diagnosis and management of paediatric headache. Part I: diagnosis. J Headache Pain. 2011;12(1):13-23.
- Spalice A, Del Balzo F, Papetti L, et al. Stroke and migraine is there a possible comorbidity? Ital J Pediatr. 2016;42:21.
- Ho TW, Edvinsson L, Goadsby PJ. CGRP and its receptors provide new insights into migraine pathophysiology. Nat Rev Neurol. 2010;6(10):573-582.
- Malik R, Winsvold B, Auffenberg E, Dichgans M, Freilinger T. The migraine–stroke connection: a genetic perspective. Cephalalgia. 2016;36(7):658-668.
- Cayir A, Turan MI, Tan H. Effect of vitamin D therapy in addition to amitriptyline on migraine attacks in pediatric patients. Braz J Med Biol Res. 2014;47(4):349-354.
- Termine C, Özge A, Antonaci F, Natriashvili S, Guidetti V, Wöber-Bingöl Ç. Overview of diagnosis and management of paediatric headache. Part II: therapeutic management. J Headache Pain. 2011;12(1):25-34.
- Ornello R, Ripa P, Pistoia F, et al. Migraine and body mass index categories: a systematic review and meta-analysis of observational studies. J Headache Pain. 2015;16:27.
- Lin Y-K, Lin G-Y, Lee J-T, et al. Associations between sleep quality and migraine frequency: a cross-sectional case-control study. Medicine (Baltimore). 2016;95(17):e3554.
- Roach REJ, Helmerhorst FM, Lijfering WM, Stijnen T, Algra A, Dekkers OM. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. 2015;(8):CD011054. doi:1002/14651858.CD011054.pub2.
- Hu X, Zhou Y, Zhao H, Peng C. Migraine and the risk of stroke: an updated meta-analysis of prospective cohort studies. Neurol Sci. 2017;38(1):33-40.
- Gelfand AA, Fullerton HJ, Jacobson A, et al. Is migraine a risk factor for pediatric stroke? Cephalalgia. 2015;34(14):1252-1260.
- Lanthier S, Carmant L, David M, Larbrisseau A, de Veber G. Stroke in children: the coexistence of multiple risk factors predicts poor outcome. Neurology. 2000;54(2):371-378.
- Serrano F, Arauz A, Uribe R, Becerra LC, Mantilla K, Zermeño F. Long-term follow-up of patients with migrainous infarction. Clin Neurol Neurosurg. 2018;165:7-9.
- Baena CP, D’Amico RC, Slongo H, Brunoni AR, Goulart AC, Benseñor I. The effectiveness of aspirin for migraine prophylaxis: a systematic review. Sao Paulo Med J. 2017;135(1):42-49.