
Peer Reviewed
Triamterene Kidney Stones
 A 64-year-old woman with a history of recurrent kidney stones presented with severe left flank pain radiating to the left lower quadrant of 4 days’ duration. She brought with her a large fragmented 70-mg stone that she had passed in urine. Her medications included hydrochlorothiazide, 25 mg/triamterene, 37.5 mg.
A 64-year-old woman with a history of recurrent kidney stones presented with severe left flank pain radiating to the left lower quadrant of 4 days’ duration. She brought with her a large fragmented 70-mg stone that she had passed in urine. Her medications included hydrochlorothiazide, 25 mg/triamterene, 37.5 mg.
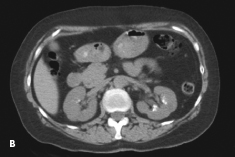
An abdominal radiograph (A) and a CT scan of the kidneys, ureters, and bladder (B) showed bilateral renal calcifications. On the right, the largest was 3 mm, and on the left, multiple punctate calcifications were evident. Urinalysis was positive for trace blood and trace leukocytes. The analysis of the stone revealed triamterene composition. The patient underwent successful placement of ureteral stents to help passage of the stones followed by lithotripsy.
In the 1970s, triamterene was the major cause of drug-induced renal calculi.1 In a 1980 study, the estimated annual incidence of triamterene lithiasis was 1 per 1500 users of triamterene/hydrochlorothiazide.2 Triamterene was found in 0.4% (181 of 50,000) of renal calculi submitted for analysis.2 This percentage has probably changed in recent years because indinavir and sulfadiazine are now the most common causes of drug-containing renal stones.1,3 Triamterene is still responsible, however, for many drug-induced calculi.
 Both unchanged triamterene and its metabolites, hydroxytriamterene and sulfate ester of hydroxytriamterene, are present in triamterene stones.4 Up to one third of triameterene stones consist entirely of triamterene.2,5 In the remainder, triameterene formed the nucleus of the stone or was deposited with calcium oxalate or uric acid; this finding suggests that in the majority of cases, triamterene lithiasis develops in persons who have had renal stones.2 It becomes incorporated into existing stone nidi by binding to the protein matrix found in all kidney stones.6
Both unchanged triamterene and its metabolites, hydroxytriamterene and sulfate ester of hydroxytriamterene, are present in triamterene stones.4 Up to one third of triameterene stones consist entirely of triamterene.2,5 In the remainder, triameterene formed the nucleus of the stone or was deposited with calcium oxalate or uric acid; this finding suggests that in the majority of cases, triamterene lithiasis develops in persons who have had renal stones.2 It becomes incorporated into existing stone nidi by binding to the protein matrix found in all kidney stones.6
Treatment consists of discontinuation of the medication and lithotripsy, because the calculi cannot be dissolved by pH manipulation.3 On plain radiographs, triamterene stones are—as in this case—faintly radio-paque and are less dense than calcium oxalate stones. They are more detectable on a CT scan of the kidneys, ureters, and bladder.
This case illustrates the need to be cautious in the use of triamterene, particularly in patients who are predisposed to nephrolithiasis or who have a prior history of kidney stones, to avoid the formation of new calculi. This caution applies even when triamterene is used in combination with hydrochlorothiazide.2
1. Daudon M, Jungers P. Drug-induced renal calculi: epidemiology, prevention and management. Drugs. 2004;64:245-275.
2. Ettinger B, Oldroyd NO, Sorgel F. Triamterene nephrolithiasis. JAMA. 1980;244:2443-2445.
3. Matlaga BR, Shah OD, Assimos DG. Drug-induced urinary calculi. Rev Urol. 2003;5:227-231.
4. Sorgel F, Ettinger B, Benet LZ. The true composition of kidney stones passed during triamtrene therapy. J Urol. 1985;134:871-873.
5. Carr MC, Prien EL Jr, Babayan RK. Triamterene nephrolithiasis: renewed attention is warranted. J Urol. 1990;144:1339-1340.
6. Werness PG, Bergert JH, Smith LH. Triamterene urolithiaisis: solubility, pH, effect on crystal formation, and matrix binding of triamterene and its metabolites. J Lab Clin Med. 1982;99:254-262.