
Peer Reviewed
The Influence of Chronic Stress on the Development of Psychiatric Conditions
ABSTRACT: A 20-year-old woman with a history of bipolar disorder (BD), posttraumatic stress disorder (PTSD), and borderline personality disorder (BPD) presented to the emergency department with suicidal ideation. This report compares her clinical course with that of her twin brother, who also had received a BD diagnosis but grew up in a less stressful environment than his sister. It also describes the possible genetic and environmental etiologic factors associated with BD, PTSD, BPD, and other psychiatric conditions. Chronic stress is strongly associated with the development of these conditions; pathologic processes involving the effect of stress hormones and neurotransmitters on the brain and central nervous system are described, along with pharmacologic and nonpharmacologic approaches to reducing chronic stress in persons with BD and other psychological disorders.
KEYWORDS: Bipolar disorder, posttraumatic stress disorder, borderline personality disorder, chronic stress, stress reduction, mental health
_________________________________________________________________________________________________________________________________________
A 20-year-old woman was admitted to the hospital after presenting to the emergency department (ED) for suicidal ideation. She had a history of bipolar disorder (BD), attention-deficit/hyperactivity disorder, posttraumatic stress disorder (PTSD), anxiety, and borderline personality disorder (BPD).
Patient History
She had a recent history of hour-long periods of increased energy, flights of ideas, and other manic symptoms. Once a month, prior to menstruation, she said she experiences a manic episode in which she feels that she has “tons of energy and would like to get everything done” but always feels that she does not have enough time to do so. She stated that these episodes usually last 1 to 2 hours. She also reported difficulty concentrating, a short attention span, and forgetfulness.
The patient also described experiencing frequent flashbacks of her traumatic experiences and said that these flashbacks impact her life negatively. For instance, she said that taking showers had become extremely uncomfortable for her because she is reminded of her past trauma. She reported being too anxious to even leave her own house and go to work. She reported having difficulty sleeping due to her racing thoughts, and waking up several times every night. She reported having had difficulty sleeping since childhood, a condition that had worsened after she had begun living in foster care group homes.
She also reported a history of chronic pain that spares only the toes ever since having sustained a traumatic head injury at age 14, when she had been physically assaulted in a group home while taking a bath. For example, she described that whenever she flexes her head downward, pain radiates to her arms and her entire back. She also reported having chronic knee pain that is refractory to intra-articular corticosteroid injections. She said that her chronic pain is refractory to acetaminophen and ibuprofen alone, adding that only acetaminophen-hydrocodone and hydromorphone relieve her pain. She rated her current pain at 8 on a 10-point scale. She had run out of pain medication 4 days ago and had not taken any since then.
The patient had an extensive history of suicide attempts beginning at age 8, and she most recently had attempted suicide 6 months ago by overdosing on acetaminophen.
Her current medications included aripiprazole, lamotrigine, fluoxetine, ibuprofen, and acetaminophen-hydrocodone.
She had a history of substance abuse, including a 5 pack-year smoking history before having quit the previous year, and she reported having regularly consumed alcohol and used marijuana until the previous year, as well as having experimented with cocaine.
The patient has an extensive family history of psychiatric illness. She reported that she and her twin brother both received a diagnosis of BD at age 5. Her father and mother also have BD; additionally, both parents and her twin have major depressive disorder, anxiety, and obsessive-compulsive disorder.
This report compares our patient’s clinical course with that of her twin brother, who also received a BD diagnosis but lived in a relatively less stressful environment than did his sister during his adolescence. It also describes the possible genetic and environmental etiologic factors associated with BD, PTSD, BPD, and other psychiatric conditions. Chronic stress is strongly associated with the development of these conditions; pathologic processes involving the effect of stress hormones and neurotransmitters on the brain and central nervous system are described, along with pharmacologic and nonpharmacologic approaches to reducing the chronic stress in persons with BD and other psychological disorders.
Physical Examination
The patient was evaluated at bedside by the psychiatric team. She was awake, alert, and oriented to date, place, and person, and she was very cooperative during the interview. She had a somnolent affect yet was hyperverbal. She cried numerous times during the interview.
The patient’s vital signs were as follows: temperature, 36.7°C; blood pressure, 126/76 mm Hg; pulse, 86 beats/min; and respiratory rate, 18 breaths/min. She was obese, with a body mass index of 44.9 kg/m2.
Physical examination revealed multiple well-healed scars on the upper and lower extremities bilaterally. The patient had no visible head injuries. Cardiovascular and abdominal examination findings were normal. Tenderness was elicited on the upper and lower back, as well as in the knee joints. The patient exhibited decreased range of motion of her back, and pain was elicited upon motion. Muscle strength was 5/5 in all extremities, and all reflexes were intact.
NEXT: Laboratory Testing, Bipolar Disorder, and more
Laboratory Testing
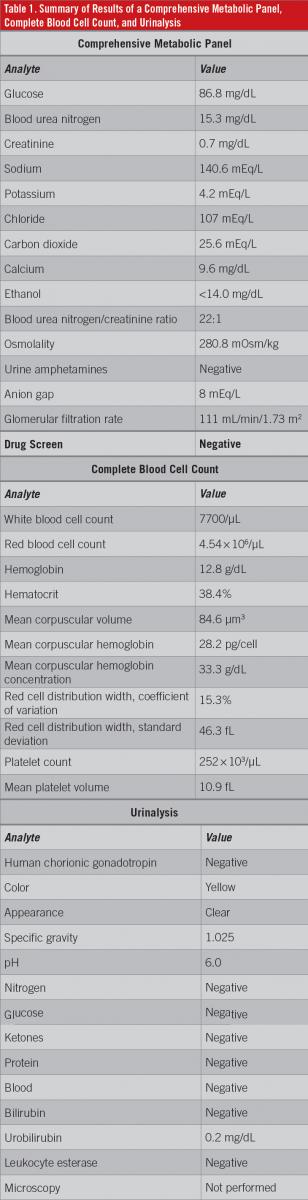
At presentation in the ED, an electrocardiogram showed no abnormalities. Toxicology screening was negative for alcohol, barbiturates, benzodiazepine, cannabinoids, cocaine, phencyclidine, opiates, amphetamines, and tricyclic antidepressants. Results of a comprehensive metabolic panel, a complete blood cell count, and urinalysis are summarized in Table 1.
The patient was assessed for BD via bedside interview and the Mood Disorder Questionnaire (MDQ) screening instrument. The interview focused on the criteria used to diagnose BD (ie, mood, behavior, cognitive abilities, psychological symptoms, and physiologic symptoms). The patient’s MDQ score was strongly positive at 12/13. (Her twin’s MDQ score, in contrast, was 3/13).
Bipolar Disorder
This patient had numerous concomitant psychiatric conditions. She had received a BD diagnosis at a young age, and she later developed other psychiatric conditions during adolescence and adulthood; at presentation, she also had PTSD and BPD.
BD, also known as manic-depressive illness, is a recurrent and episodic mood disturbance that ranges from mania to severe depression.1 It is typically associated with cognitive disturbances such as delusions, an inability to concentrate, racing thoughts, and a false belief of superiority. It is also associated with psychotic features such as hallucinations.1 BD is diagnosed clinically; diagnostic tests for it do not yet exist. BD has several clinical subtypes, including type 1 (full manic episodes), type 2 (hypomanic episodes but major depressive episodes), and bipolar-type schizoaffective disorder (manic episodes occurring together with psychotic symptoms).
Studies of families and twins have revealed a strong genetic component associated with BD, with heritability estimates in the range of 60% to 85%.1 The development of BD is also influenced by environmental factors such as chronic stress—long-term emotional pressure over which an individual perceives he or she has no control. Experiencing traumatic situations, especially over a prolonged period, can trigger the development of BD, especially in genetically susceptible individuals, due to the prolonged exposure of the brain to neurotransmitters such as cortisol that are associated with chronic stress.
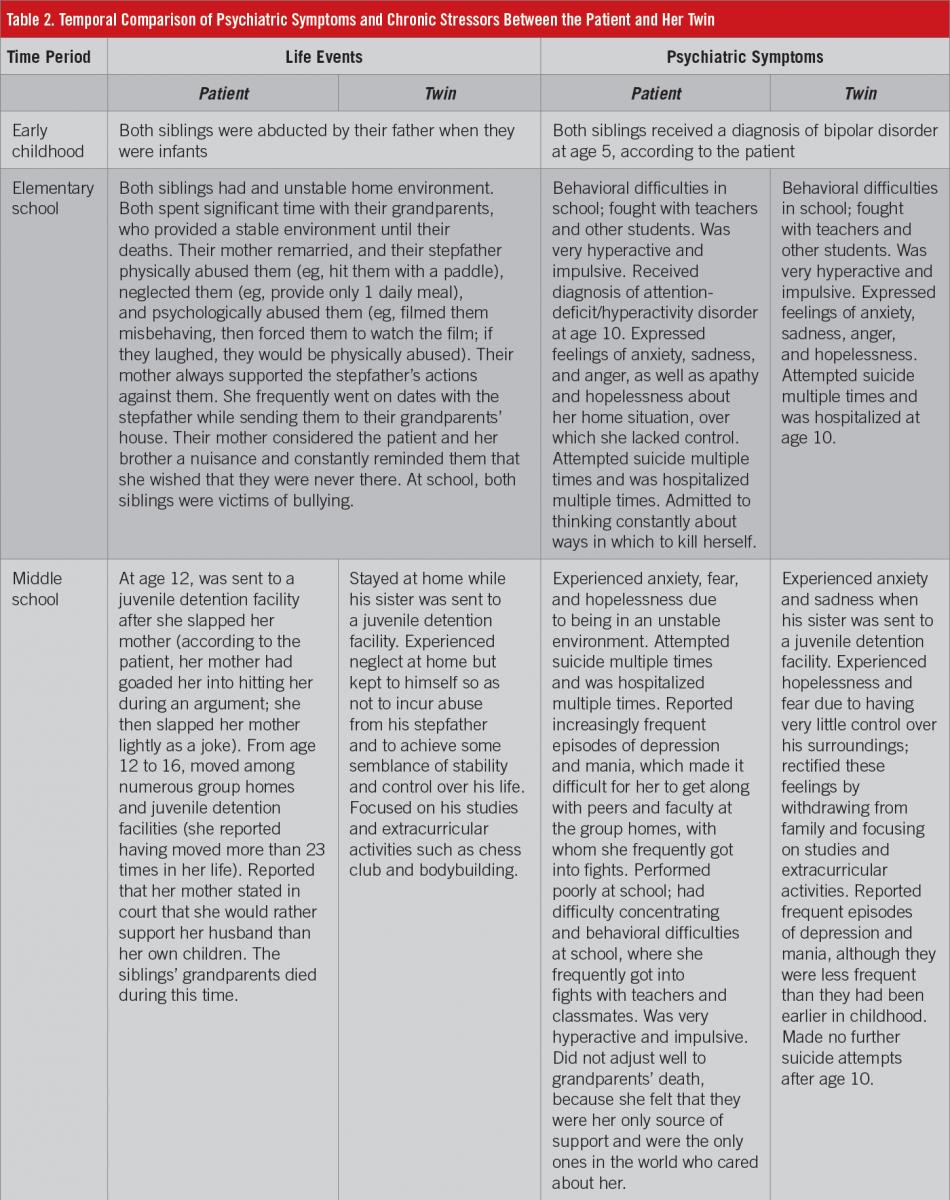
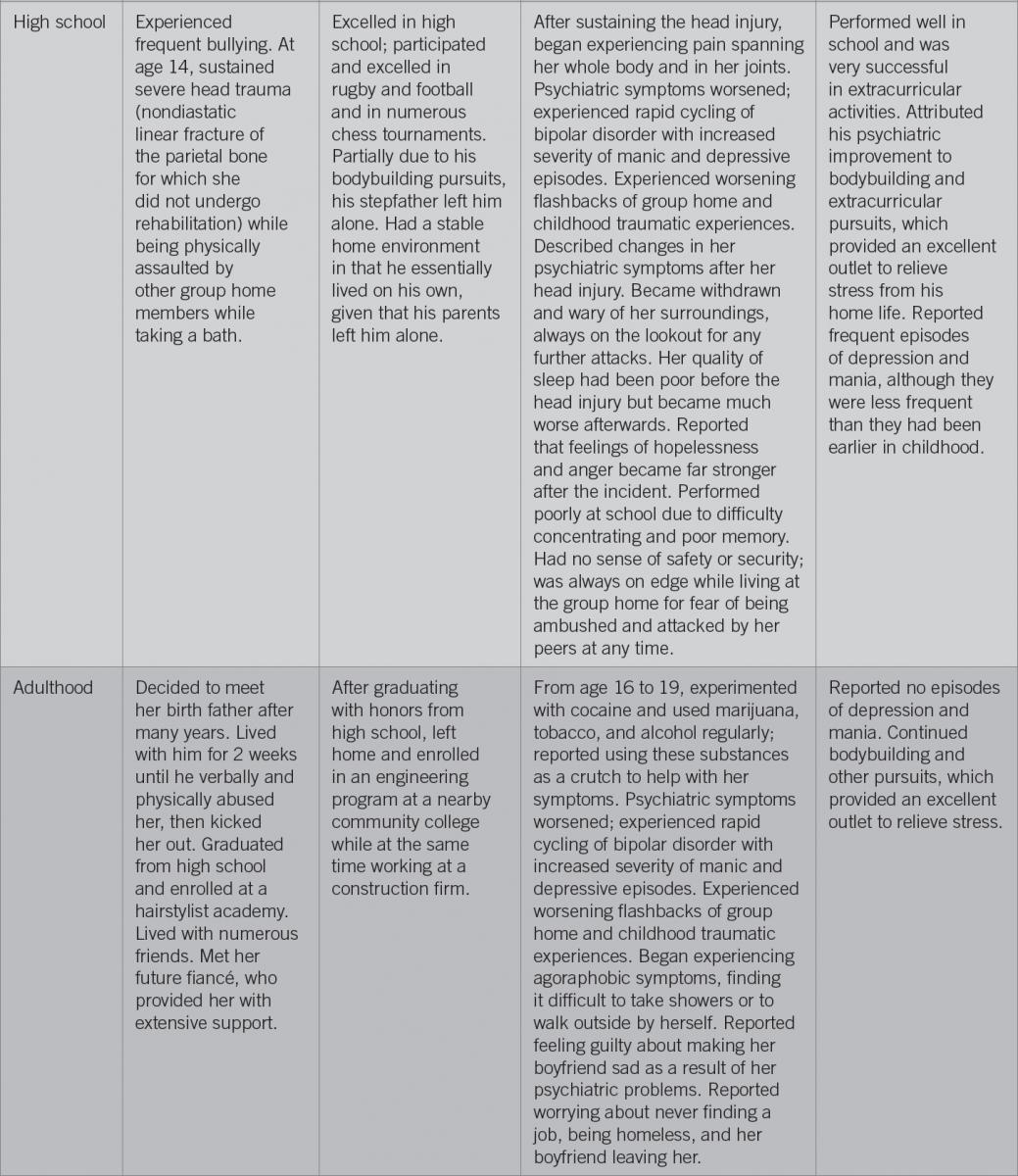
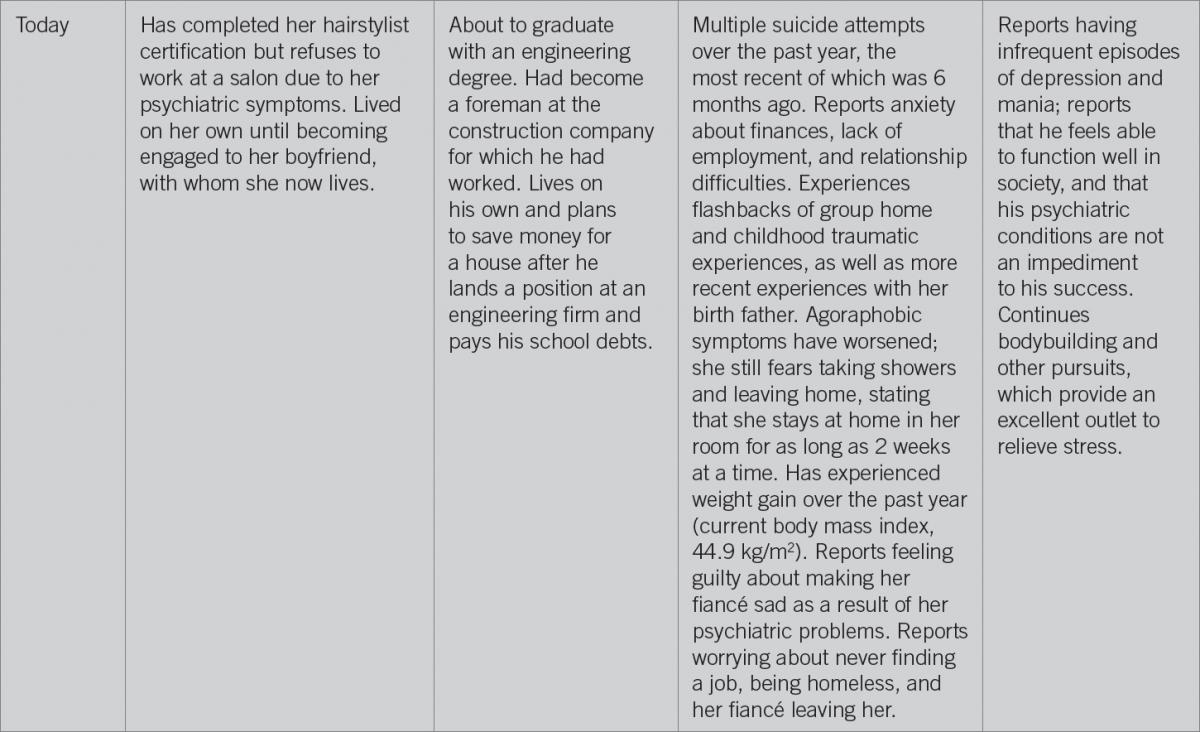
Our patient’s family history demonstrates the strong genetic component associated with BD (Table 2). Her mother, father, and twin brother had the condition. The presentation of BD differed among each family member, however. The patient meets most of the criteria for BD and was currently in the rapid cycling phase of the condition, as evidenced by her more than 4 distinct episodes of depression, mania, or hypomania occurring in the past year.2 Her twin, however, meets only one criterion, mild depression. Essentially, he no longer has BD. This discrepancy might be explained by the different levels of chronic stress that either twin faced in their life.
Posttraumatic Stress Disorder
PTSD is a psychiatric condition that is triggered by witnessing or experiencing a traumatic event such as a sexual assault, warfare, a motor vehicle accident, or other threat to a person’s life.3 Symptoms include increased arousal, changes in how a person thinks or feels, and flashbacks—experiencing disturbing thoughts, feelings, or dreams related to the traumatic event, which elicit mental and physical distress. Flashbacks can be triggered by cues related to the traumatic incident. Not all persons who experience a traumatic event develop PTSD.3 Complex PTSD (C-PTSD), a variant of PTSD, is triggered by chronic or long-term exposure to emotional trauma over which an individual has no control nor hope for escape.4 Individuals who experience domestic/childhood emotional, physical, or sexual abuse; entrapment or kidnapping; slavery; long-term imprisonment and/or torture; and long-term exposure to stressful situations can develop C-PTSD. Symptoms can include persistent sadness, suicidality, explosive anger, and inhibited anger.
As in BD, genetics plays a role in the development of PTSD, albeit to a lesser extent. Studies of families and twins have revealed a strong genetic component associated with PTSD, with heritability estimates in the range of 30% to 40%.5 Single-nucleotide polymorphisms in FKBP5 (a gene that has been associated with the mechanism of dissociation during a traumatic situation) have been linked to increased susceptibility to the development of PTSD.5
Our patient has symptoms of PTSD, as evidenced by her agoraphobia and flashbacks of her past traumatic events (Table 2). Moreover, she displays symptoms of C-PTSD, such as persistent sadness, suicidality, and explosive anger. Her twin, on the other hand, only displayed these symptoms during childhood but not during high school and through to adulthood.
Borderline personality disorder
BPD is a psychiatric disorder characterized by unstable relationships with others, an unstable sense of self, and unstable emotions.6 Persons with BPD usually have a fear of abandonment and a feeling of emptiness and frequently engage in dangerous behavior. Substance abuse, depression, eating disorders, and suicide are associated with BPD.6
Genetics plays a role in the development of BPD, the estimated heritability of which is 40%.7 Approximately 42% of variations in BPD features have been found to be attributable to genetic influences and 58% to environmental influences.7
Our patient has symptoms of BPD, including compulsive behavior, impulsivity, self-destructive behavior, anger, anxiety, general discontent, guilt, loneliness, mood swings, and a history of suicide attempts (Table 2).
NEXT: Chronic Stress and the Brain, The Clinical Approach
Chronic Stress and the Brain
Findings from a significant number of published studies in the literature support the idea that chronic stress is linked with the development of BD, PTSD, and BPD. For example, approximately 30% to 50% of adults with BD report having had traumatic/abusive experiences in childhood,8 and 39% of persons with BD have comorbid PTSD.9 One theory about this connection implicates maladaptive brain remodeling due to chronically increased levels of stress hormones and neurotransmitters as a cause of BD.10,11
The brain processes stress in 3 main areas: the amygdala, the hippocampus, and the prefrontal cortex. The prefrontal cortex is the center for critical and rational thought, and the amygdala is responsible for processing emotions.12 The hippocampus, the central organ for learning, converts working memory found in the prefrontal cortex into long-term memory through neuronal remodeling by connecting this new information with what is already known.12
The brain responds to stress by activating the amygdala; the amygdala then activates the hypothalamic-pituitary-adrenal (HPA) axis, causing an elevation in levels of circulating cortisol. A proinflammatory state can also activate the HPA axis through interleukin 6 (IL-6) synthesis.13
The neurons in the prefrontal cortex, amygdala, and hippocampus have more corticosteroid receptors than do other areas of the brain.10 Through the binding of these receptors by cortisol, the brain can process the intensity of physical and psychological stressors acting upon the body. During situations of acute stress, cortisol increases hippocampal activity and leads to long-term potentiation and memory formation.10 Acute elevations of cortisol increases prefrontal cortical activity, promoting concentration.10 Acute stimulation of these corticoid receptors also is responsible for the fight-or-flight response mediated by the amygdala, allowing the brain to quickly process information and thereby react to life-threatening situations.10
Chronic stress leads to overactivation of the amygdala and the HPA axis, leading to a constantly elevated cortisol level.10 This chronic overactivation leads to increased neuronal density of the amygdala through dendritic branching,14 resulting in amygdala hyperactivity, which contributes to the increased anxiety and heightened emotional responses associated with not only BD, but also PTSD and BPD. Meanwhile, hippocampal and prefrontal cortical neurons are overstimulated by chronic exposure to cortisol and are then shut down to prevent their death, resulting in atrophy of the hippocampus and the prefrontal cortex.15
Atrophy of the prefrontal cortex leads to impairment of regulating behavior, thought, and emotion. Because the prefrontal cortex is responsible for promoting concentration, impairment can lead to a lack of concentration. The prefrontal cortex also allows for flexible regulation of behavior, which is useful for responding to a changing environment, inhibiting inappropriate actions, and monitoring errors and the need to modify behavior strategies accordingly.16 Overactivation of the amygdala coupled with atrophy of the prefrontal cortex therefore can lead to increased aggression, impulsivity, and impaired judgment,12 which are characteristics associated with BD, PTSD, and BPD.
Atrophy of the hippocampus leads to impairments in memory and learning difficulties.12 Cortisol impairs neurogenesis within the hippocampus, thus inhibiting the formation of new memories. Overactivation of the amygdala along with impairment of the hippocampus results in individuals focusing more on the emotions they feel rather than on obtaining new information, causing those who are exposed to a stressor to fixate on one aspect of what has triggered the stressor rather than on learning more about the stressor.12 This results in worry, feelings of resentment, and a reduction of mental agility. This maladaptive brain remodeling is especially prominent in children with developing brains who are exposed to chronic stress.12
These physiologic processes, along with impaired neuroplasticity and long-term potentiation in the brain, result in a string of neurologic symptoms mirroring those of BD and other psychiatric disorders in which involvement of these brain structures is implicated. One group of authors16 found that chronic stress resulted in a 16% decrease in apical dendritic spine density in medial prefrontal cortex pyramidal neurons, resulting in reduced neuroplasticity, for which dendritic spines play a crucial role.
Atrophy and neuroplasticity impairments of the prefrontal cortex result in increased aggression and changes in dopaminergic activity, as well as changes in decision-making strategies, from that of a flexible strategy to a habit-based strategy, increasing the likelihood of addiction, hopelessness, and apprehension.17 Atrophy of the hippocampus results in decreased long-term potentiation, leading to impaired working and spatial memory.18 Supporting this theory are the results of imaging studies done on patients with BD that reveal decreased volume of the hippocampus and prefrontal cortex.19 Our patient’s symptoms also support this theory—she reported impaired memory, addictive behaviors, apprehension, and hopelessness, as well as depression and mania, associated with fluctuating dopaminergic activity.
A proinflammatory state can also activate the HPA axis. A considerable number of patients with BD have circulating monocytes that are in a proinflammatory state.20 These monocytes express a set of 19 inflammation-related genes—the PDE4B-associated proinflammatory gene expression signature. This gene expression can also be found in the monocytes of children of patients with BD and particularly in children developing a mood disorder; thus the proinflammatory state of monocytes precedes the occurrence of mood disorder symptoms.20 Accordingly, persons who have increased expression of PDE4B-associated proinflammatory genes therefore might be more susceptible to developing BD.
Changes in levels of tumor necrosis factor α, another proinflammatory molecule, in the central nervous system also have been found to be associated with mood symptoms in humans.21 Chronic psychological stress, such as constant activation of the fight-or-flight response, can activate the proinflammatory genes associated with BD. Moreover, arachidonic acid is elevated in a proinflammatory state, which leads to IL-6 synthesis; elevated IL-6 stimulates the HPA axis to increase cortisol release, which can contribute to BD and PTSD.13
The Clinical Approach
Clinicians should consider prioritizing stress reduction when managing patients with BD, PTSD, and BPD. Cognitive behavioral therapy is extremely effective in this regard in that it allows patients to become aware of their inaccurate or negative thinking so that they can view challenging situations more clearly and respond to them in a more effective way.22
Clinicians should also identify patients’ stressors and do their best to help rectify them. For example, patients with financial difficulties can be referred to a social worker to help with managing finances, finding a job, or applying for financial assistance. Patients in abusive environments should receive help to leave such environments.
Medical therapy to address sleep difficulties and other comorbid conditions also can help reduce stress, as was seen in the case of our patient, whose symptoms improved after adjustments to her treatment regimen and relocation to a less stressful environment.
During her hospital stay, her medication regimen was modified with the addition of trazodone, 50 mg at bedtime, and bupropion, 150 mg once a day. Her dosage of aripiprazole was increased from 10 mg/d to 15 mg/d, and her dosage of ibuprofen was increased from 500 mg every 8 hours as needed to 800 mg every 8 hours as needed. Fluoxetine and acetaminophen-hydrocodone were discontinued. Nonpharmacologic therapy included outpatient cognitive behavioral therapy.
Three months after her hospitalization, while following her new medication regimen, the patient’s symptoms had greatly improved. She reported being much calmer and being able to focus better, and her agoraphobia had diminished such that she now felt comfortable going outside and was now able to pursue her hairstyling career. She also reported that her neuropathic pain had diminished greatly; before, she had relied only on acetaminophen-hydrocodone to relieve her pain but now was able to manage without opioid medications. She now lives in a stable environment with her fiancé and his parents and sees a therapist regularly on a biweekly basis.
Pwint Phyu, MD, is a resident physician at Larkin Community Hospital in South Miami, Florida.
Rhaisa Dumenigo, MD, is an attending physician at Larkin Community Hospital in South Miami, Florida.
Juan D. Oms, MD, is the director of the Psychiatry Residency Program at Larkin Community Hospital in South Miami, Florida.
Luxhman Gunaseelan, MS-III, is a medical student at Saba University School of Medicine in Saba, Caribbean Netherlands.
Golbon Foroughi, MS-IV, is a medical student at Saba University School of Medicine in Saba, Caribbean Netherlands.
Syed A. A. Rizvi, PhD, is a professor in the Department of Pharmaceutical Sciences, College of Pharmacy, at Nova Southeastern University in Fort Lauderdale, Florida.
References:
- Craddock N, Sklar P. Genetics of bipolar disorder. Lancet. 2013;381(9878):1654-1662.
- Fountoulakis KN, Kontis D, Gonda X, Yatham LN. A systematic review of the evidence on the treatment of rapid cycling bipolar disorder. Bipolar Disord. 2013;15(2):115-137.
- Coughlin SS, McNeil RB. Overview of post-traumatic stress disorder. In: Coughlin SS, ed. Post-Traumatic Stress Disorder and Chronic Health Conditions. Washington, DC: American Public Health Association; 2013:1-36.
- Busuttil W. Complex post-traumatic stress disorder: a useful diagnostic framework? Psychiatry. 2009;8(8):310-314.
- Cornelis MC, Nugent NR, Amstadter AB, Koenen KC. Genetics of post-traumatic stress disorder: review and recommendations for genome-wide association studies. Curr Psychiatry Rep. 2010;12(4):313-326.
- Koenigsberg HW, Siever LJ. Borderline personality disorder. In: Fink G, ed. Encyclopedia of Stress. Vol 1. 2nd ed. New York, NY: Academic Press; 2007:348-350.
- Amad A, Ramoz N, Thomas P, Jardri R, Gorwood P. Genetics of borderline personality disorder: systematic review and proposal of an integrative model. Neurosci Biobehav Rev. 2014;40:6-19.
- Brietzke E, Kauer-Sant’anna M, Jackowski A, et al. Impact of childhood stress on psychopathology. Rev Bras Psiquiatr. 2012;34(4):480-488.
- Krishnan KRR. Psychiatric and medical comorbidities of bipolar disorder. Psychosom Med. 2005;67(1):1-8.
- McEwen BS, Nasca C, Gray JD. Stress effects on neuronal structure: hippocampus, amygdala, and prefrontal cortex. Neuropsychopharmacology. 2016;41(1):3-23.
- Berk M, Kapczinski F, Andreazza AC, et al. Pathways underlying neuroprogression in bipolar disorder: focus on inflammation, oxidative stress and neurotrophic factors. Neurosci Biobehav Rev. 2011;35(3):804-817.
- Goleman D. Emotional Intelligence: Why It Can Matter More Than IQ. New York, NY: Bantam Books; 2006.
- McNamara RK, Lotrich FE. Elevated immune-inflammatory signaling in mood disorders: a new therapeutic target? Exp Rev Neurother. 2012;12(9):1143-1161.
- Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. 2009;10(6):434-445.
- Hains AB, Arnsten AF. Molecular mechanisms of stress-induced prefrontal cortical impairment: implications for mental illness. Learn Mem. 2008;15(8):551-564.
- Radley JJ, Morrison JH. Repeated stress and structural plasticity in the brain. Ageing Res Rev. 2005;4(2):271-287.
- Mineur YS, Prasol DJ, Belzung C, Crusio WE. Agonistic behavior and unpredictable chronic mild stress in mice. Behav Genet. 2003;33(5):513-519.
- Mizoguchi K, Yuzurihara M, Ishige A, Sasaki H, Chui D-H, Tabira T. Chronic stress induces impairment of spatial working memory because of prefrontal dopaminergic dysfunction. J Neurosci. 2000;20(4):1568-1574.
- Maletic V, Raison C. Integrated neurobiology of bipolar disorder. Front Psychiatry. 2014;5:98.
- Padmos RC, Van Baal GCM, Vonk R, et al. Genetic and environmental influences on pro-inflammatory monocytes in bipolar disorder: a twin study. Arch Gen Psychiatry. 2009;66(9):957-965.
- Berk M, Kapczinski F, Andreazza AC, et al. Pathways underlying neuroprogression in bipolar disorder: focus on inflammation, oxidative stress and neurotrophic factors. Neurosci Biobehav Rev. 2011;35(3):804-817.
- Searson R, Mansell W, Lowens I, Tai S. Think Effectively About Mood Swings (TEAMS): a case series of cognitive–behavioural therapy for bipolar disorders. J Behav Ther Exp Psychiatry. 2012;43(2):770-779.