
A Collection of Conditions With Dermatologic Manifestations
Keratosis Follicularis
Jacqueline Bullock, BS, PA-S
Keiser University, Fort Lauderdale, Florida
Syed A. A. Rizvi, PhD, and Sultan S. Ahmed, MD
Nova Southeastern University, Fort Lauderdale, Florida
Jose Mendez, DO
Fort Lauderdale, Florida
Gerardo F. Ferrer, MD
Miami, Florida
Jose D. Suarez, MD
Westchester General Hospital, Miami, Florida
Jasmin Ahmed, BS
Spartan Health Sciences University, Vieux Fort, St Lucia
A 14-year-old boy presented with a chronic rash located on his neck and upper back areas. The rash was causing the patient persistent and mild pruritus without exudates.
History. The patient had a past psychiatric history of unspecified psychosis with prodromal symptoms, which are prominent in patients who receive a schizophrenia diagnosis later in life. During the initial evaluation, the patient also reported having commanding auditory hallucinations and delusions. The delusions were numerous but mainly were of the paranoid and grandiose type. Furthermore, the boy’s grandmother disclosed a positive family history of mental illness in both of the patient’s parents; because of the debilitating nature of the parents’ mental disorder, the patient had been raised by his grandmother.
Physical examination. Vital signs were as follows: body mass index, 25.4 kg/m2; pulse, 63 beats/min and regular; respiration rate, 16 breaths/min; temperature, 37°C; and blood pressure, 110/65 mm Hg. His neck was supple, with a normal thyroid and no jugular distention. The lungs were clear to auscultation. Cardiac and abdominal examination findings were normal.
Dermatologic examination revealed a rash of yellow-brown papules with a warty and greasy texture on the neck and upper back (Figures 1 and 2). The lesions had mild to moderate pruritus and were negative for erythema and exudates. No blisters were noted, and the lesions were nontender.


On mental examination, the patient was cooperative but with suspicious behavior. He was poorly groomed and had fair hygiene, with a dysthymic mood and a constricted affect. His thought process was tangential, and flights of ideas were present, as well. He revealed paranoid and grandiose delusions as part of the thought content, along with perception disturbances noteworthy for auditory hallucinations of the commanding type, of which patient stated, “They tell me to harm others.” He denied any suicidal or homicidal ideation. Cognition was intact, alert, and oriented to person, place, and time.
Diagnostic tests. Laboratory tests disclosed the following: white blood cell count, 5200/µL; hemoglobin, 12.6 g/dL; hematocrit, 37.4%; aspartate aminotransferase, 16 U/L; alanine aminotransferase, 12 U/L; urea nitrogen, 11 mg/dL; creatinine, 0.56 mg/dL; glucose, 84 mg/dL; total cholesterol, 139 mg/dL; low-density lipoprotein cholesterol, 80 mg/dL; high-density lipoprotein cholesterol, 43 mg/dL; triglycerides, 79 mg/dL; platelet count, 225 × 103/µL; and total bilirubin, 0.6 mg/dL.
Skin histopathology results showed the epidermis to contain a focus of acantholysis and dyskeratosis. There was a mixed inflammatory infiltrate in the dermis beneath (Figure 3). Periodic acid–Schiff stain results were negative for pathogenic fungi.

Discussion. This patient’s rash is most consistent with keratosis follicularis (also known as Darier disease or Darier-White disease). Patients with keratosis follicularis typically have a family history of this autosomal dominant inherited condition. However, a number of cases have been reported with no clear family history of keratosis follicularis.1 Such cases are likely due to sporadic mutations or from a family member with an unrecognized mild case of keratosis follicularis.
Patients with keratosis follicularis exhibit greasy, hyperkeratotic papules with histopathologic evidence of acantholysis and dyskeratosis in seborrheic regions, and nail and mucous membrane changes.1 The lesions are located primarily in seborrheic areas such as the forehead, scalp, hairline, nasolabial folds, ears, chest, and back.2 Approximately 80% of patients have mild involvement of the flexure surfaces, including the groin, axillae, or breast creases in women. Approximately 95% of patients have skin changes on the palms.3
Keratosis follicularis is estimated to affect approximately 1 to 4 people per 100,000 worldwide, typically between the ages of 6 and 20 years, and is evenly distributed between the sexes. It is a chronic condition with exacerbations that fluctuate with triggers over time. It is caused by mutations of ATP2A2.4 This gene is responsible for encoding the sarcoplasmic/endoplasmic reticulum Ca2+-ATPase isoform 2 protein known as SERCA2, which transfers calcium from the cell into the lumen of the endoplasmic reticulum. It is not known exactly how the molecular mechanisms of ATP2A2 mutations alter the function of SERCA2.4 However, the mutations cause acantholysis and dyskeratosis of the skin via defects in protein expression, ATP hydrolysis, calcium transport, calcium binding and kinetics, and abnormal cytokeratin expression.4 Mutations in ATP2A2, in addition to causing keratosis follicularis, have been associated with neuropsychiatric conditions including epilepsy, schizophrenia, mood disorders, and learning disabilities.2,3,5
The appearance and odor of the lesions can contribute to major morbidity through psychosocial consequences.5
Differential diagnoses include seborrheic dermatitis, acrokeratosis verruciformis, benign familiar pemphigus (Hailey-Hailey disease), and transient acantholytic dermatosis (Grover disease). Histopathologic findings of acantholysis and dyskeratosis are the main features of keratosis follicularis. It most often includes a large keratin plug that usually shows focal parakeratosis overlying each lesion. Histopathologic testing can confirm the diagnosis, supported by gene sequencing to observe the mutation in ATP2A2 on chromosome 12.6
No specific treatment or cure exists for keratosis follicularis, and treatment is aimed at its symptoms. It is important to take measures to prevent flares, such as keeping the skin moisturized with keratolytics, using antiseptics to prevent infections, and minimizing perspiration. Other treatments include topical corticosteroids and topical and oral retinoids.
Surgical techniques such as dermabrasion, laser ablation, surgical excision, and photodynamic therapy have also been used, but recurrence is common.7
References:
- Tavadia S, Mortimer E, Munro CS. Genetic epidemiology of Darier’s disease: a population study in the west of Scotland. Br J Dermatol. 2002;146(1):107-109.
- Celik T, Celik U, Donmezer C, Komur M, Tolunay O, Demirtürk P. Cooccurrence of Darier’s disease and epilepsy: a pediatric case report and review of the literature. Case Rep Pediatr. 2014;2014:831398. doi:10.1155/2014/831398
- Quinlivan JA, O’Halloran LC. Dariers disease and pregnancy. Dermatol Aspects. 2013;1:1. doi:10.7243/2053-5309-1-1
- Savignac M, Edir A, Simon M, Hovnanian A. Darier disease: a disease model of impaired calcium homeostasis in the skin. Biochim Biophys Acta. 2011;1813(5):1111-1117.
- Ruiz-Perez VL, Carter SA, Healy E, et al. ATP2A2 mutations in Darier’s disease: variant cutaneous phenotypes are associated with missense mutations, but neuropsychiatric features are independent of mutation class. Hum Mol Genet. 1999;8(9):1621-1630.
- Sehgal VN, Srivastava G. Darier’s (Darier-White) disease/keratosis follicularis. Int J Dermatol. 2005;44(3):184-192.
- Dicken CH, Bauer EA, Hazen PG, et al. Isotretinoin treatment of Darier’s disease. J Am Acad Dermatol. 1982;6(4 pt 2 suppl):721-726.
NEXT: Tinea Pedis
Tinea Pedis
Joe R. Monroe, MPAS, PA
Dermatology Associates of Oklahoma, Tulsa

For more than 20 years, a 47-year-old woman had had an asymptomatic rash on the sides and bottoms of both feet. A few months before presentation, her friend had received a diagnosis of psoriasis on her feet, so the patient borrowed her friend’s topical corticosteroid cream (clobetasol) and started applying it to her own feet.
At first, the clobetasol seemed to smooth out the rough skin on her feet, but over time the redness became more widespread, moving up onto the sides of the feet, much higher than before. Then, tiny blisters began to appear on the edges of the rash, at which point she sought referral to a dermatologist.
Physical examination. The redness was striking and uniform, covering the soles and sides of the feet in one continuous sheet. The borders of the rash were fairly sharply drawn with scaly edges, which were scraped for a potassium hydroxide preparation examination, which revealed fungal hyphae too numerous to count.
Discussion. It is a little known fact, even among medical providers, that there are 3 forms of “athlete’s foot.” These include the most common type, the interdigital type, which most commonly presents with maceration between the fourth and fifth toes. The second most common is moccasin-type tinea pedis, which is what our patient had, in which the bottoms and rims of the feet are red and scaly, although most often cases are otherwise asymptomatic. Most patients who have moccasin-type tinea pedis have no idea what condition they have. The least common type of tinea pedis is the inflammatory type, presenting acutely with vesicles and pustules on the plantar instep.
When corticosteroids are used in an attempt to treat tinea pedis, the body’s immune response to the condition is blunted, allowing the organisms to flourish. In our patient’s case, the solution was obvious: Stop the corticosteroids and start oral terbinafine, 250 mg, for 1 month, plus miconazole cream twice a day. While this will not cure the tinea pedis, it will at least return the condition to its state before she applied clobetasol.
The point is that injudicious application of corticosteroid creams changes and worsens fungal infections, often making them difficult to recognize.
NEXT: Rosacea
Rosacea
Alexander K. C. Leung, MD
Alberta Children’s Hospital, University of Calgary,
Alberta, Canada
Benjamin Barankin, MD
Toronto Dermatology Centre, Toronto, Ontario, Canada

A 42-year-old woman presented with a mild periodic burning and stinging sensation on her face, facial erythema, and red papules on her cheeks that had been present for approximately 3 years. The rash was aggravated by sun exposure and ingestion of spicy foods. She had stopped wearing makeup since the appearance of the rash. She spent a lot of time outdoors gardening and hiking. Her past health history was unremarkable except for atopic dermatitis and seborrheic dermatitis. She was quite withdrawn due to embarrassment about her skin condition.
Physical examination revealed inflammatory papules and tiny pustules on an erythematous background over the cheeks. No comedones were present. The rest of the physical examination findings were unremarkable.
A clinical diagnosis of rosacea was made. The patient was treated with topical metronidazole in the morning, topical ivermectin in the evening, and low-dose doxycycline, 40 mg, once daily for 3 months, after which her skin condition had improved by more than 95%.
Discussion. Rosacea is a common chronic inflammatory skin disorder characterized by a spectrum of clinical signs, including flushing, nontransient erythema, telangiectasia, and inflammatory papulopustules affecting the central face, including the cheeks, nose, eyes, forehead, and chin.1 Four clinical subtypes have been identified: erythematotelangiectatic, papulopustular, phymatous, and ocular.2
Epidemiology. The reported prevalence is 1% to 22% of the adult population.3,4 The wide variation in the reported prevalence can be attributed to the different diagnostic criteria, different methodology (direct observation vs self-reported surveys), the studied population phototype, and cultural and social perceptions of the condition.4 The onset is usually between 30 and 50 years of age, although rarely children and adolescents may be affected.1,5 The condition is much more common in fair-skinned individuals.1,5,6 In addition, the diagnosis is often missed in patients of color, even when they have symptoms suggesting it.7 With the exception of phymatous rosacea, women are more frequently affected than men.1,8
Etiopathogenesis. Pathogenic factors include dysregulation of the innate immune system as evidenced by an increased baseline expression of cathelicidin and kallikrein 5; a defect in neuroinflammatory mechanisms; reactive oxygen species; abnormal barrier function; solar irradiation; vascular hyperactivity; and local inflammatory reactions to cutaneous microorganisms such as Staphylococcus epidermidis, Bacillus oleronius, and skin mites Demodex folliculorum and Demodex brevis.5,6,8
Predisposing factors include consumption of alcohol, hot beverages, spicy foods, nuts, chocolate, and cheese; smoking; sun exposure; extremes of temperature; irritation from topical products (eg, waterproof cosmetics); drugs (eg, vasodilators, corticosteroids, nicotinic acid); a family history of rosacea; strenuous exercise; and emotional stress.5,8,9 Menstruation and pregnancy can also exacerbate rosacea.4,5
Histopathology. Histopathologic examination of a classic lesion in erythematotelangiectatic rosacea usually shows dilation of superficial blood vessels and low-grade perivascular lymphohistiocytic infiltrate.8,10
In papulopustular rosacea, histopathologic examination of a papule usually reveals prominent perivascular and perifollicular infiltrate in the superficial and mid-dermis consisting of lymphocytes, neutrophils, and plasma cells, while histopathologic examination of a pustule reveals superficial accumulations of neutrophils.8,10
Histopathologic findings in phymatous rosacea include sebaceous gland hyperplasia, follicular plugging, telangiectasia, pronounced dermal thickening and fibrosis, and a large amount of dermal mucin.8,10
Clinical manifestations. Any of the 4 rosacea subtypes can coexist in a patient. Our patient had predominantly papulopustular rosacea.
Erythematotelangiectatic rosacea is the most common subtype and is characterized by persistent erythema of the central face, transient facial erythema (flushing), erythema congestivum, telangiectasia, skin sensitivity (burning, stinging, tingling sensation), and roughness and scaling of skin.5,8 The perioral and periocular areas are typically spared.5
Papulopustular rosacea, the second most common subtype, is characterized by persistent central facial erythema, along with inflammatory dome-shaped erythematous papules and tiny surmounting pustules on the central face.4,8 Edema is sometimes present.11 The inflammation may extend outward to form plaques. Comedones are characteristically absent, and affected patients are significantly older than the typical acne patient.
Phymatous rosacea is characterized by skin and sebaceous hypertrophy with irregular surface nodularities. The affected skin surface tends to be pitted with large, patulous, expressive follicles.11 Significant telangiectases are often present over the affected area. The nose (rhinophyma) is the most commonly affected site, although the chin/jaw (gnatophyma), forehead (metophyma), eyelids (blepharophyma), and ears (otophyma) may also be affected. This subtype occurs mainly in men.1,8
Ocular rosacea may manifest as conjunctival hyperemia, foreign body sensation, burning or stinging, abnormal tearing, light sensitivity, blurred vision, lid margin telangiectases, anterior blepharitis, cicatricial conjunctivitis, and formation of a chalazion or hordeolum.8,10 Ocular rosacea is significantly more common in the younger age group.12
Diagnosis and differential diagnosis. The diagnosis is usually a clinical one and rarely requires histologic confirmation. The differential diagnosis includes acne vulgaris, corticosteroid-induced acneiform eruption, perioral dermatitis, seborrheic dermatitis, chronic photodamage, keratosis pilaris rubra faceii, dermatomyositis, and lupus erythematosus.5,8
Complications and prognosis. Rosacea is a potentially disfiguring condition that can be socially embarrassing given its chronic nature and its tendency to affect the face, a highly visible area. The condition can impair one’s body image and self-esteem and can have a negative impact on the quality of life.13 Affected patients are at risk for migraine, depression, dyslipidemia, cardiovascular disease, hypertension, thyroid cancer, and basal cell carcinoma.4,8,14,15
Although symptoms may wax and wane and the condition can burn out in some cases, roseacea is usually progressive in the long run.1 In this regard, men usually progress to the advanced stages of the disease more often than women.5
Treatment. There is no cure for rosacea. Treatment is aimed at controlling symptoms. In general, affected patients may benefit from gentle skin cleansing, frequent use of moisturizers/barrier repair formulations, regular use of broad-spectrum sunscreens when outdoors, and cosmetic camouflage.1,6 Exacerbating factors such as consumption of alcohol, hot beverages, spicy foods, nuts, and cheese, as well as irritating topical products (eg, waterproof cosmetics), sun exposure (especially during hours of peak UV intensity), extremes of temperature, and physical and emotional stress should be avoided if possible.6,12,16
For erythematotelangiectatic rosacea, the erythema can be treated with topical brimonidine or topical oxymetazoline, while telangiectases are best treated with a laser or light-based device.1,6,16-18 Treatment of papulopustular rosacea includes topical metronidazole, topical azelaic acid, topical ivermectin, topical sulfacetamide-sulfur, oral isotretinoin, and oral tetracyclines, alone or in combination.1,5,15,17,18 Early cases of phymatous rosacea can be treated with oral tetracyclines or oral isotretinoin, while advanced cases may require treatment with ablative lasers, electrosurgery, or surgical debulking.5 Patients with ocular rosacea benefit from oral tetracyclines; for significant involvement or lack of treatment response, consideration of referral to an ophthalmologist for evaluation and management should be considered.
REFERENCES:
- Chang BP, Kurian A, Barankin B. Rosacea: an update on medical therapies. Skin Therapy Lett. 2014;19(3):1-4.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584-587.
- Moustafa F, Hopkinson D, Huang KE, Feldman S. Prevalence of rosacea in community settings. J Cutan Med Surg. 2015;19(2):149-152.
- Tan J, Berg M. Rosacea: current state of epidemiology. J Am Acad Dermatol. 2013;69(6 suppl 1):S27-S35.
- Tüzün Y, Wolf R, Kutlubay Z, Karakuş O, Engin B. Rosacea and rhinophyma. Clin Dermatol. 2014;32(1):35-46.
- Moustafa FA, Sandoval LF, Feldman SR. Rosacea: new and emerging treatments. Drugs. 2014;74(13):1457-1465.
- Al-Dabagh A, Davis SA, McMichael AJ, Feldman SR. Rosacea in skin of color: not a rare diagnosis. Dermatol Online J. 2014;20(10):13.
- Dahl MV. Rosacea: pathogenesis, clinical features, and diagnosis. UpToDate. http://www.uptodate.com/contents/rosacea-pathogenesis-clinical-features-and-diagnosis. Updated January 23, 2017. Accessed January 31, 2017.
- Abram K, Silm H, Maaroos H-I, Oona M. Risk factors associated with rosacea. J Eur Acad Dermatol Venereol. 2010;24(5):565-571.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol. 2015;72(5):749-758.
- Kennedy Carney C, Cantrell W, Elewski BE. Rosacea: a review of current topical, systemic and light based therapies. G Ital Dermatol Venereol. 2009;144(6):673-688.
- Reinholz M, Tietze JK, Kilan K, et al. Rosacea – S1 guideline. J Dtsch Dermatol Ges. 2013;11(8):768-780.
- Cresce ND, Davis SA, Huang WW, Feldman SR. The quality of life impact of acne and rosacea compared to other major medical conditions. J Drugs Dermatol. 2014;13(6):692-697.
- Duman N, Ersoy Evans S, Atakan N. Rosacea and cardiovascular risk factors: a case control study. J Eur Acad Dermatol Venereol. 2014;28(9):1165-1169.
- Li W-Q, Zhang M, Danby FW, Han J, Qureshi AA. Personal history of rosacea and risk of incident cancer among women in the US. Br J Cancer. 2015;113(3):520-523.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part II. Topical and systemic therapies in the treatment of rosacea. J Am Acad Dermatol. 2015;72(5):761-770.
- Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 2: a status report on topical agents. Cutis. 2013;92(6):277-284.
- van Zuuren EJ, Fedorowicz Z. Interventions for rosacea. JAMA. 2015;314(22):2403-2404.
NEXT: Tuberous Sclerosis Complex
Tuberous Sclerosis Complex
Meghan A. Helm, BS
Albany Medical College, Albany, New York
Ankit Gor, MD
Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, New York
An 18-year-old woman presented for evaluation and treatment of facial papules that had been increasing in number and becoming more widespread (Figures 1 and 2). Her classmates had been teasing her because of her appearance. She was accompanied by a legal guardian, because her mother was undergoing inpatient treatment for neuropsychiatric disease.

Figure 1. Multiple firm brown papules were symmetrically distributed over the face and showed confluence in the nasolabial folds.

Figure 2. The patient’s lesions were extensive; some were dome-shaped, whereas others had a filiform appearance mimicking an acrochordon (skin tag).
History. The patient had noted a gradual increase in the number of facial lesions over many years but otherwise had been in good health. The facial lesions were not painful but were bothersome because of their appearance. In addition to her mother’s history of neuropsychiatric illness, there was a family history of seizure disorder.
Physical examination. Numerous brown papules were noted on the face, with confluence in the nasolabial folds. An indurated flesh-colored shagreen patch was noted on her back. The presence of multiple angiofibromas and shagreen patch led to a clinical diagnosis of tuberous sclerosis complex (TSC).
Several of the largest facial lesions were removed. Biopsy results confirmed the lesions to be angiofibromas, thereby confirming the TSC diagnosis (Figures 3 and 4).
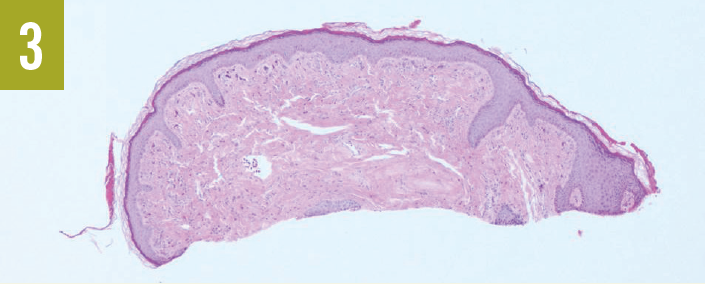
Figure 3. Biopsy revealed a dome-shaped lesion that was devoid of viral cytopathic effect. (Hematoxylin-eosin–stained sections; magnification x40.)
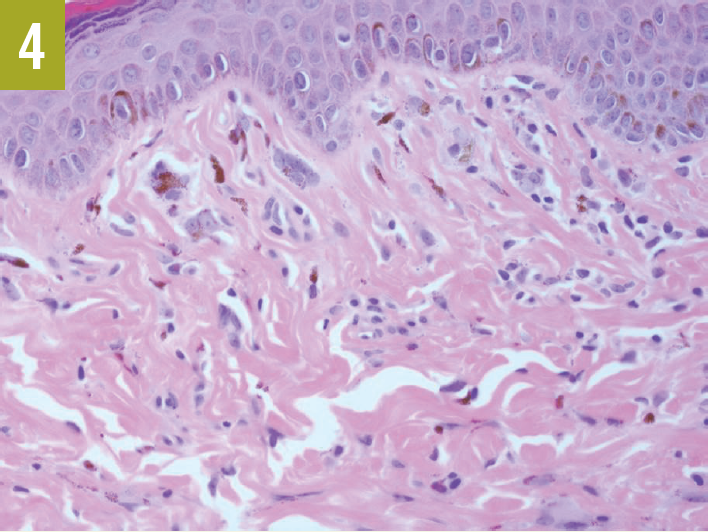
Figure 4. Higher-power magnification (x400) revealed the thickened collagen bundles and stellate fibrocytes that are characteristic of an angiofibroma.
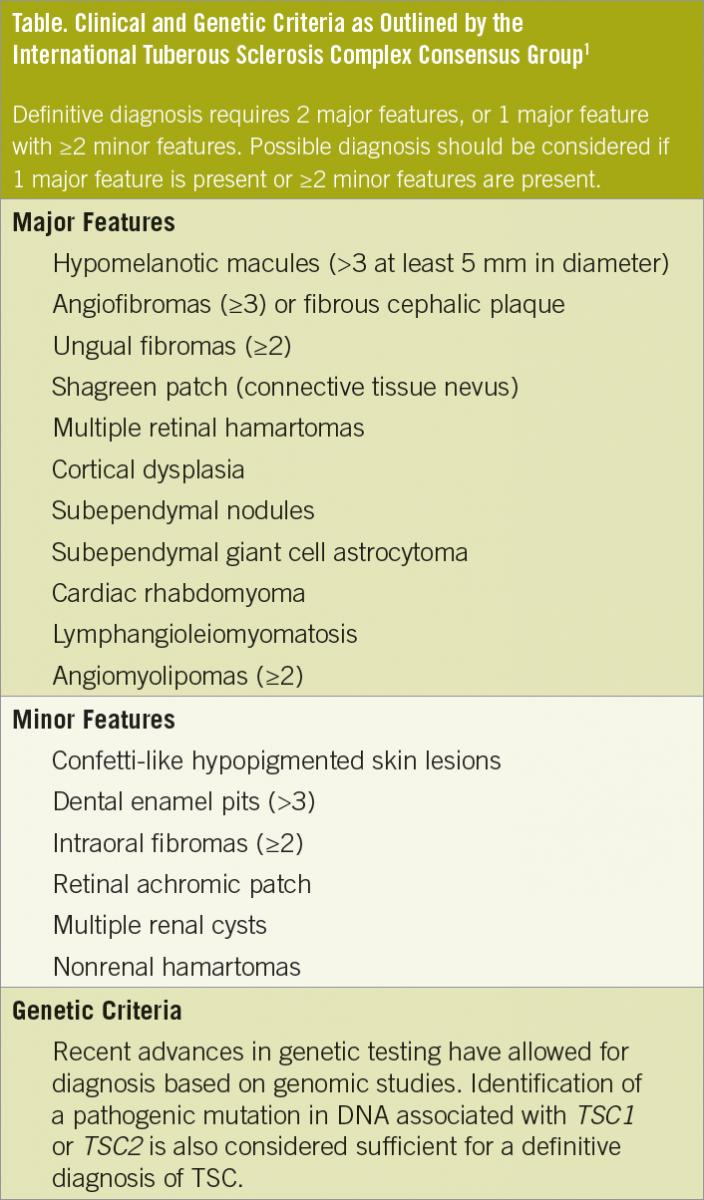
Discussion. The multiple extensive lesions of our patient are characteristic of the facial angiofibromas (adenoma sebaceum) of TSC.1 TSC is associated with a variety of other cutaneous, neurologic, and systemic manifestations (Table). Affected patients develop the characteristic lesions, which include angiofibromas, connective tissue nevi (shagreen patch), and confetti-like hypochromic lesions. The angiofibromas usually develop in late childhood and gradually increase in number. Seizures, brain tumors, and neuropsychiatric disorders may also develop.
Brain imaging studies are important to identify subependymal giant-cell tumors (SGCTs). SGCTs should be resected if they are acutely symptomatic and are surgically accessible.2,3 SGCTs can lead to focal neurologic deficits, behavioral changes, hydrocephalus, and seizures. Children with TSC should be evaluated for autism spectrum disorders, intellectual disabilities, and neuropsychiatric problems. Some patients may develop debilitating pulmonary disease, including diffuse interstitial fibrosis and lymphangioleiomyomatosis.
Treatment of lesions typically includes surgical removal by shave excision, snip excision, curettage, or laser ablation. Topical everolimus is a newer option that targets the abnormal mTOR signaling thought to be pathogenic in TSC.4 n
References:
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013;49(4):243-254.
- Karenfort M, Kruse B, Freitag H, Pannek H, Tuxhorn I. Epilepsy surgery outcome in children with focal epilepsy due to tuberous sclerosis complex. Neuropediatrics. 2002;33(5):255-261.
- Goh S, Butler W, Thiele EA. Subependymal giant cell tumors in tuberous sclerosis complex. Neurology. 2004;63(8):1457-1461.
- Dill PE, De Bernardis G, Weber P, Lösch U. Topical everolimus for facial angiofibromas in the tuberous sclerosis complex: a first case report. Pediatr Neurol. 2014;51(1):109-113.