
Bilateral Adrenal Hemorrhage in a Patient With Antiphospholipid Syndrome
Authors:
Osama Mukarram, MD; Adnan Haider, MD; Ahmed Khan, MD; and Mary Mok, MD
Texas Tech University Health Sciences Center at the Permian Basin, Odessa, Texas
Citation:
Mukarram O, Haider A, Khan A, Mok M. Bilateral adrenal hemorrhage in a patient with antiphospholipid syndrome. Consultant. 2017;57(2):128-129.
A 33-year-old man presented with bilateral flank pain associated with nausea and vomiting 10 days after having undergone an uncomplicated laparoscopic cholecystectomy. He denied having had fever, chills, hematuria, or dysuria.
History. In the last 2 years, he had had multiple emergency department visits for episodic abdominal pain. He had developed left iliac vein thrombosis resulting in stent placement 5 years prior at another facility and had received a diagnosis of antiphospholipid syndrome (APLS). He had been lost to follow-up and had prematurely discontinued anticoagulation.
Physical examination. His abdomen was soft, with mild diffuse tenderness. No physical examination findings were suggestive of appendicitis or pyelonephritis. His vital signs were as follows: temperature, 37.6°C; heart rate, 83 beats/min; respiratory rate, 18 breaths/min; and blood pressure, 114/75 mm Hg.
Diagnostic tests. Laboratory test results showed a white blood cell count of 6050/µL (reference range, 4500-11,000/µL), a hemoglobin level of 13.9 g/dL (reference range, 14.0-17.5 g/dL), a hematocrit level of 40.6% (reference range, 41%-50%), and a platelet count of 87.6 × 103/µL (reference range, 150-350 × 103/µL). Results of a comprehensive metabolic panel showed a sodium concentration of 122 mEq/L (reference range, 136-142 mEq/L), a potassium concentration of 2.9 mEq/L (reference range, 3.5-5.0 mEq/L), a chloride concentration of 83 mEq/L (reference range, 96-106 mEq/L), and a creatinine level of 1.0 mg/dL (reference range, 0.6-1.2 mg/dL). Results of liver function tests were normal.
Furthermore, the prothrombin time was 13.8 s (reference range, 9-12 s), the activated partial thromboplastin time was 61.2 s (reference range, 24-35 s), and the thrombin time was 16.1 s (reference value, <20 s). Results of urinalysis with microscopic examination and urine toxicology testing did not show any abnormalities.
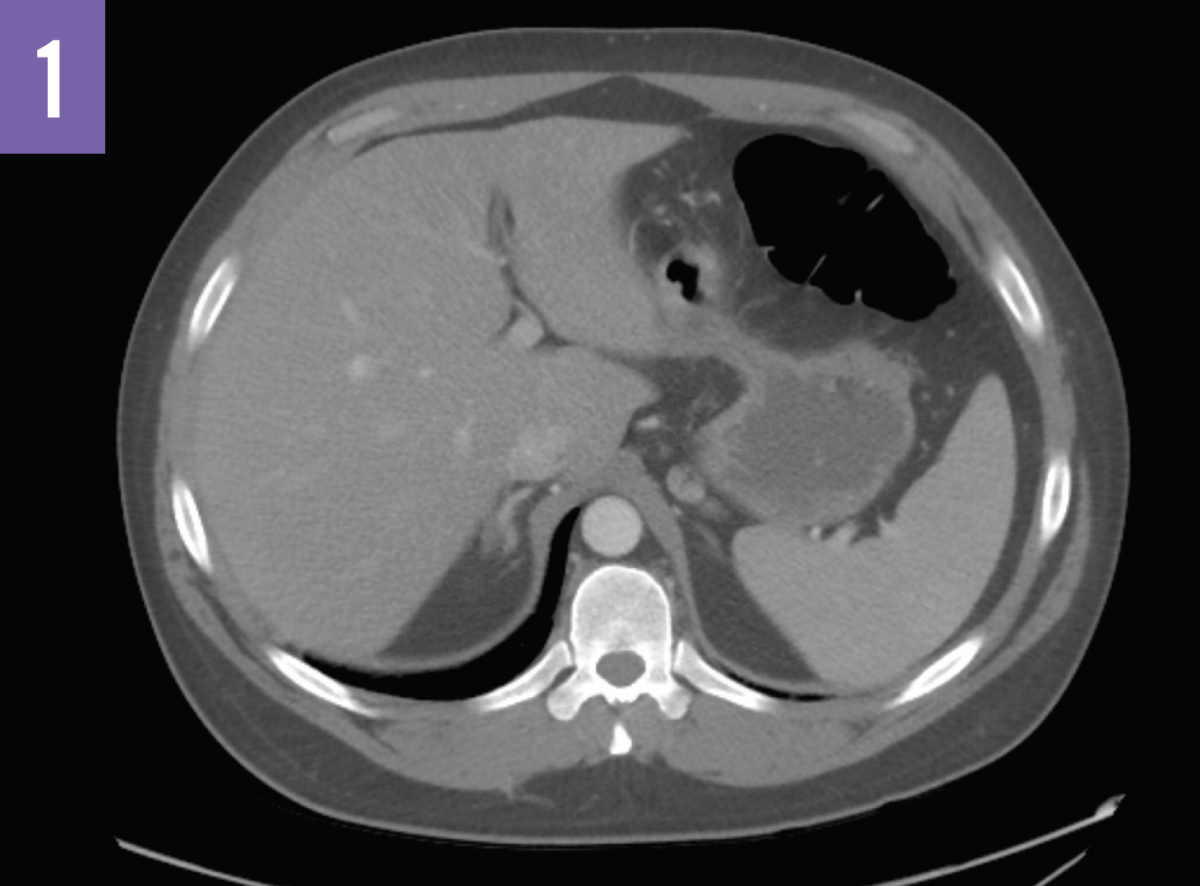
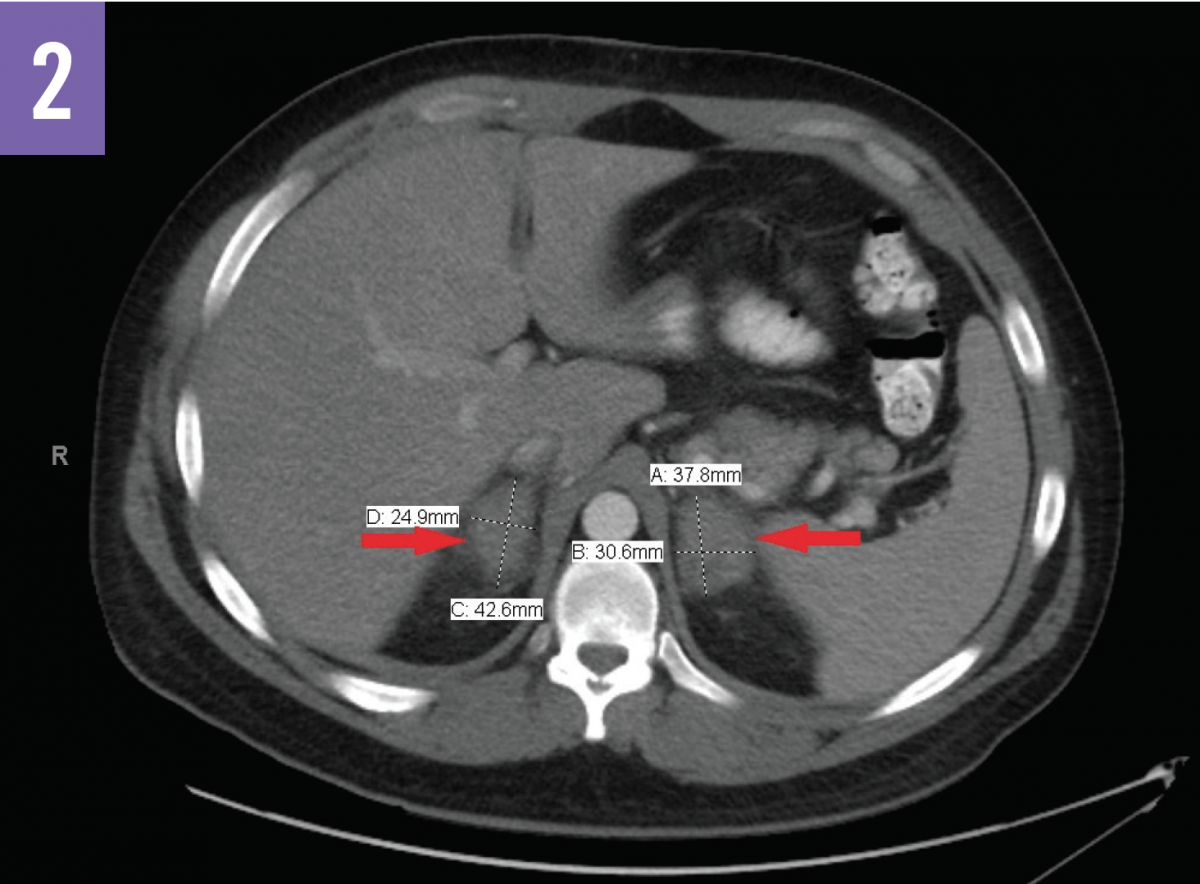
Computed tomography (CT) scans of the abdomen (Figures 1 and 2) showed acute bilateral adrenal gland enlargement. Compared with abdominal CT scans done 10 days prior for acute cholecystitis, these findings were new and highly suggestive of acute bilateral adrenal hemorrhage. His serum cortisol level was found to be <0.16 µg/dL (reference range, 5-25 µg/dL). The patient remained hemodynamically stable. Results of repeated laboratory tests for APLS, including anticardiolipin antibody and lupus anticoagulant testing, were positive for APLS.
The patient was started on a regimen of warfarin, with a target international normalized ratio (INR) of 3.0 to 3.5, and corticosteroid replacement therapy with hydrocortisone and fludrocortisone.
Outcomes >>
Discussion. APLS accounts for less than 1% of cases of adrenal insufficiency.1 The pathogenesis of adrenal insufficiency in APLS is not completely understood. It is thought that a high level of cholesterol in the adrenal glands attracts the antiphospholipid antibodies, which in turn leads to thrombosis and hemorrhage. Furthermore, the rich blood flow into and slow transit of blood out of the adrenal glands predisposes them to stasis and eventually adrenal hemorrhage, especially in hypercoagulable states such as APLS.2
Clinical manifestations of the disease are apparent when 90% or more of the adrenal cortices are destroyed or dysfunctional.1 Chronic abdominal pain is a well-documented presentation of APLS. Abdominal manifestations of APLS other than acute adrenal hemorrhage include Budd-Chiari syndrome and hepatic, splenic, and intestinal infarctions. The proposed pathogenesis for these abdominal manifestations includes arterial thrombosis and venous thrombosis.3
Acute bilateral adrenal hemorrhage requires prompt diagnosis and empirical treatment with corticosteroids to avoid the development of hemodynamic instability and shock. Usual daily doses range between 150 and 200 mg of hydrocortisone.4 These dosages are tapered down over a few days to replacement regimens of 15 to 30 mg hydrocortisone or equivalent in divided doses, along with mineralocorticoids.
The prognosis of acute bilateral adrenal hemorrhage remains good so long as patients undergo appropriate treatment, including anticoagulation and corticosteroid replacement therapy. The suggested INR target for these patients is between 3.0 and 3.5 when using warfarin. The degree of involvement of the adrenal glands at initial presentation determines the need for lifelong corticosteroid replacement.1
Outcome of the case. At 8 weeks of follow-up, our patient remained hemodynamically stable, and his abdominal pain had resolved. He continues to be on anticoagulation and corticosteroid replacement regimens.
Given the extensive involvement of the adrenal glands in this case, we anticipate that the patient will benefit from lifelong corticosteroid replacement therapy.
REFERENCES:
- Ramon I, Mathian A, Bachelot A, et al. Primary adrenal insufficiency due to bilateral adrenal hemorrhage-adrenal infarction in the antiphospholipid syndrome: long-term outcome of 16 patients. J Clin Endocrinol Metab. 2013;98(8):3179-3189.
- Mo GP, Germaine P, Mastoris J, Henry DH. Adrenal hemorrhage associated with antiphospholipid antibody syndrome. Community Oncol. 2005;2(3):265-269.
- Choi BG, Jeon HS, Lee SO, Yoo WH, Lee ST, Ahn DS. Primary antiphospholipid syndrome presenting with abdominal angina and splenic infarction. Rheumatol Int. 2002;22(3):119-121.
- Shenker Y, Skatrud JB. Adrenal insufficiency in critically ill patients. Am J Respir Crit Care Med. 2001;163(7):1520-1523.