
Peer Reviewed
Bilobed Benign Pulmonary Papillary Adenoma
Authors:
Rayhaan M. Akram, MD
Department of Internal Medicine, Spectrum Health/Michigan State University, Grand Rapids, Michigan
Cynthia L. Cookingham, MD
Department of Pathology, Spectrum Health/Michigan State University, Grand Rapids, Michigan
Marc R. McClelland, MD
Department of Pulmonology and Critical Care Medicine, Spectrum Health/Michigan State University, Grand Rapids, Michigan
Citation:
Akram RA, Cookingham CL, McClelland MR. Bilobed benign pulmonary papillary adenoma [published online October 24, 2019]. Consultant360.
A 74-year-old woman presented for evaluation of enlarging pulmonary nodules in the left lower lobe that had been identified on surveillance imaging. The patient had a 50 pack-year smoking history and moderate to severe chronic obstructive pulmonary disease. Approximately a year and a half ago, she had been evaluated for dyspnea, cough, occasional night sweats, and a weight loss of approximately 9 kg over a few years.
At that time, computed tomography (CT) scans of the thorax demonstrated a 3.4-cm noncalcified density within the lingula of the lung; a 1.3-cm noncalcified lesion at the left lower lobe; a smaller 0.6-cm noncalcified lesion within close proximity to the 1.3-cm lesion; and calcified mediastinal and hilar lymphadenopathy (Figure 1).

Subsequent fluorodeoxyglucose positron emission tomography (PET) scanning revealed hypermetabolism of both the lingular mass and the 1.3-cm nodule in the left lower lobe periphery. The 0.6-cm nodule was below the resolution for the PET scan. Biopsy of an airway lesion within the lingula and a cytology specimen from bronchial washings showed atypical carcinoid, pathologic stage 1B, (T2a, N0, M0). Several days later, results of a percutaneous CT-guided biopsy of the left lower lobe nodule were consistent with a normal intrapulmonary lymph node.
The patient underwent surgical resection of the lingular mass with lobectomy. Pathology results showed atypical carcinoid with clear margins and no regional lymph node involvement. She had a prolonged postoperative hospital course due to mucus plugging, which improved with therapeutic bronchoscopy and suctioning. Surveillance imaging was continued for the remaining nodules at the left lung base.
On the next CT imaging study at 6 months, the nodules that were in close proximity to each other appeared to have enlarged and had become confluent (Figure 2). The confluent bi-lobed nodule was 1.5x1.0x1.7 cm, enlarged from 1.3 cm and 0.6 cm, respectively, about 6 months prior.

CT-guided biopsy of the lesion was again obtained. Histology results now showed papillary epithelial proliferation with papillary cores lined by cuboidal to low columnar nonciliated epithelial cells (Figure 3). There was absence of mitotic activity, and immunohistochemistry results were negative for chromogranin and synaptophysin, findings most consistent with papillary adenoma. The findings were morphologically distinct from her prior atypical carcinoid.
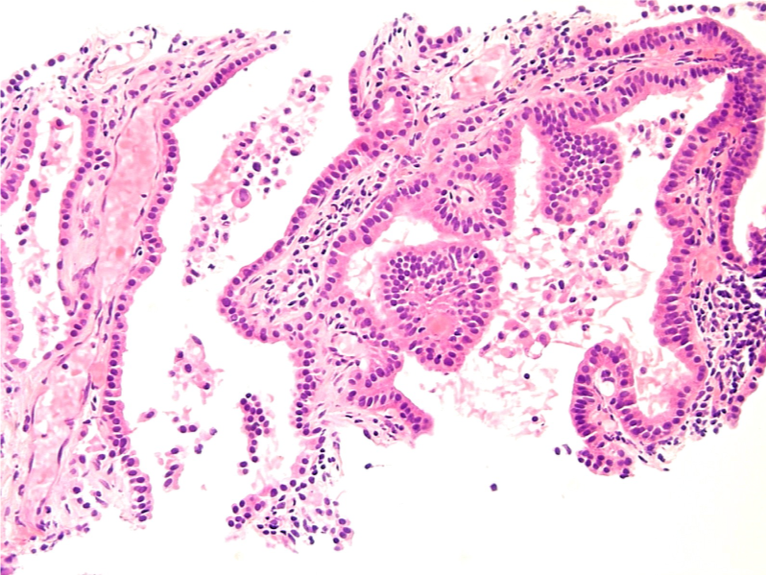
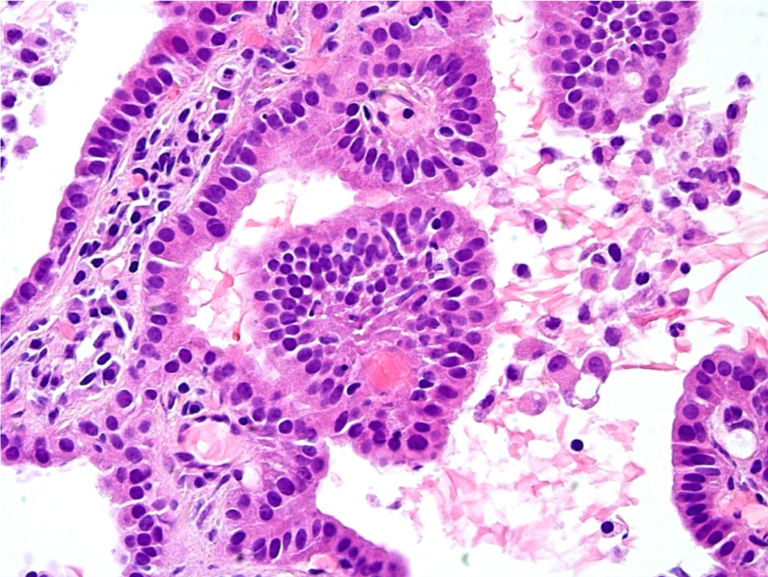
Figure 3. Histology results of the bilobed confluent nodule shows papillary profiles with well-formed papillary cores lined by cuboidal to low columnar nonciliated epithelial cells.
Given the indolent nature of papillary adenoma, the plan is to continue surveillance with no immediate intervention.
DISCUSSION
Papillary adenoma of the lungs is a rare disease, with fewer than 30 published reports in the English-language medical literature. It was first named by Fantone and colleagues in 1982,1 in a patient who had developed a complex papillary growth pattern in the right lung comprised of nonciliated cuboidal and columnar epithelium, with characteristics of club cell and type II pneumocyte differentiation. Prior to this, in 1980, Spencer and colleagues described 19 noninvasive papillary neoplasms, of which two resembled club cells on light microscopy.2 Type II pneumocytes are cuboidal and clustered epithelial cells located at the alveolar walls that secrete pulmonary surfactant and serve as precursors to type I pneumocytes. Club cells (formerly Clara cells) are nonciliated columnar/cuboidal cells with secretory granules and are located at the distal bronchioles. These cells secrete a component of surfactant, degrade toxins, and serve as reserve cells of bronchial epithelium. Papillary adenomas are thought to arise from precursor multipotential stem cells that can differentiate into type II pneumocytes and club cells. Most reported cases have shown type II pneumocyte differentiation.3
Papillary adenomas are generally small, with an average size of 2.0 cm.4 They have no lobar predominance and are most commonly located at the periphery of the lung, as in our patient’s case, although Lin and colleagues report a case occurring in the central portion of the lung.5 Most papillary adenomas have been solitary lesions, with few exceptions. Kurotaki and colleagues describe multiple lesions of papillary adenoma, up to 2 mm in diameter, found in all lobes in a 13-year-old boy with neurofibromatosis.6
Reported cases of papillary adenomas show a 2-to-1 male predominance.4 The patients range in age from 2 months to 78 years, with a mean age in the 30s.7 Our patient’s case is unique in that it involves a 74-year-old woman who had two adjacent nodules of papillary adenoma that became confluent.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis includes malignant and benign neoplasms. Papillary adenoma is a histologically distinct entity. It is well-defined with a predominance of papillary structures with fibrovascular cores. The cells are cuboidal or columnar and lacking marked atypia and very rarely with mitosis. Vessels within the fibrous stroma are thin-walled and dilated.1 The immunohistochemical profile of papillary adenoma is also a distinguishing feature. The cells react positively with antibodies to surfactant apoproteins, thyroid transcription factor 1, epithelial membrane antigen, pan cytokeratin, and cytokeratin 7.4 Reports have indicated that napsin A is also a useful marker for type II pneumocytes.5 The papillary adenoma epithelial cells are negative for carcinoembryonic antigen, chromogranin, and synaptophysin. Additionally, the reported cases have been negative for EGFR, KRAS, and BRAF mutations.4
Given our patient’s history of atypical carcinoid, ruling out metastasis and/or recurrence was of utmost importance. Carcinoid tumors with papillary features, as well as papillary adenoma with carcinoid features, have been described in the literature.8,9 The papillary adenomas described in such cases were all negative for chromogranin, similar to our patient’s case, which helped differentiate it from carcinoid. Additionally, the morphology of the lesion in our patient’s case was distinct from her previous atypical carcinoid mass.
Similar to papillary adenoma, alveolar adenoma is well-circumscribed and located at the lung periphery. However, alveolar adenomas contain variably sized cysts with proteinaceous material, which are not present in papillary adenomas. Sclerosing hemangioma of the lung is a rare, benign tumor that has epithelial origin similar to papillary adenoma. Additionally, it is usually well-circumscribed with a papillary growth pattern. However, it also predominantly features solid, hemorrhagic, and sclerotic patterns, which distinguish it from a papillary adenoma.9,10
Two subtypes of lung adenocarcinoma, papillary adenocarcinoma and bronchioloalveolar carcinoma, can both contain papillary structures, but these cells are generally larger than those in papillary adenoma and exhibit marked nuclear atypia with increased mitotic activity and necrosis. Additionally, these cells generally stain positive for carcinoembryonic antigen. Papillary adenoma is distinguished from metastatic papillary neoplasms by the lack of mitotic activity, necrosis, and other features of malignancy.4,9
PROGNOSIS
The malignant potential of papillary adenoma is unclear. Given the lack of marked atypia, low mitosis, and low Ki-67 proliferation rate, the disease is largely considered to be benign. However, 4 cases have shown local histologic invasion into adjacent vessels, capsule, pleura, or parenchyma.2,4,10,11 There have been no reported cases of distant metastases or recurrence after surgical resection. Therefore, authors have suggested that it is a tumor of intermediate malignant potential.4 The prognosis is quite favorable, and the primary mode of treatment has been surgical resection. Of note, Kurotaki and colleagues reported no progression of papillary adenoma after 6 years in the 13-year-old boy with multiple lesions and neurofibromatosis, despite no surgical resection.6
Given our patient’s comorbidities and complicated postoperative course of her prior surgical resection, it was elected to continue close follow-up with surveillance imaging with no immediate plan for intervention
REFERENCES:
- Fantone JC, Geisinger KR, Appelman HD. Papillary adenoma of the lung with lamellar and electron dense granules: an ultrastructural study. Cancer. 1982;50(12):2839-2844.
- Spencer H, Dail DH, Arneaud J. Non-invasive bronchial epithelial papillary tumors. Cancer. 1980;45(6):1486-1497.
- Kuwahara M, Nagafuchi M, Rikimaru T, Iwasaki A, Shirakusa T. Pulmonary papillary adenoma. Gen Thorac Cardiovasc Surg. 2010;58(10):542-545.
- Cornejo KM, Shi M, Akalin A, Uy K, Cagle PT, Fraire AE. Pulmonary papillary adenoma: a case report and review of the literature. J Bronchology Interv Pulmonol. 2013;20(1):52-57.
- Lin X-Y, Han Q, Wang E-H, Zhang Y. Pulmonary papillary adenoma presenting in central portion: a case report. Diagn Pathol. 2015;10:190.
- Kurotaki H, Kamata Y, Kimura M, Nagai K. Multiple papillary adenomas of type II pneumocytes found in a 13-year-old boy with von Recklinghausen’s disease. Virchows Archiv A Pathol Anat Histopathol. 1993;423(4):319-322.
- Frey A, Alatassi H, Wiese TA, Fraig M, Yang X. Cytomorphologic findings and differential diagnosis of pulmonary papillary adenoma: a case report and literature review. Diagn Cytopathol. 2016;44(6):543-54
- Choi IH, Han J, Moon JW, Choi YS, Lee K-J. A rare case of pulmonary papillary adenoma in old aged woman: a brief case report. Korean J Pathol. 2014;48(1):66-6
- Hegg CA, Flint A, Singh G. Papillary adenoma of the lung. Am J Clin Pathol. 1992;97(3):393-397.
- Mori M, Chiba R, Tezuka F, et al. Papillary adenoma of type II pneumocytes might have malignant potential. Virchows Arch. 1996;428(3):195-200.
- Dessy E, Braidotti P, Del Curto B, et al. Peripheral papillary tumor of type-II pneumocytes: a rare neoplasm of undetermined malignant potential. Virchows Arch. 2000;436(3):289-295.