
AUTHOR:
Samuel Louie, MD
Professor of Medicine, Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine; and Director, UC Davis Asthma Network (UCAN) at UC Davis Health, Sacramento, California
CITATION:
Louie S. Lies, damned lies, and asthma. Consultant. 2018;58(12):336-342.
Aminophylline suppositories, cocaine nasal packs, and potassium iodide were commonly prescribed for asthma in 1963 when Claude A. Frazier, MD, wrote a thoughtful essay on the do’s and don’ts in treating allergic asthma in Consultant.1 How times have changed! Dr Frazier left us with several clinical observations that are prophetic. He was correct in asserting in his introduction that “allergic asthma is a problem disease; its capricious nature defies control and keeps the health of the asthmatic always in a precarious state. And, improper treatment can make the asthma worse.” His wisdom preceded the proliferation of consensus guidelines, beginning with the National Institutes of Health National Asthma Education and Prevention Program (NIH-NAEPP) Expert Panel Report (EPR-1) in 1991.2 Here I offer an updated list of do’s and don’ts and a perspective from one clinician’s experience with difficult-to-control asthma since 1998.
Lies, Damned Lies, and Statistics
I assert that practicing clinicians have been unintentionally hoodwinked by “lies, damned lies, and statistics” in the institutional, national, and international consensus guidelines that promote the illusion that asthma is a single disease that responds homogeneously to inhaled corticosteroids (ICSs) and discourage the professional initiative and independent thinking necessary to conduct a “clinical trial of one” in favor of evidenced-based treatment recommendations.
Evidence-based medicine attempts to take statistical analysis from well-designed and well-conducted clinical trials—the “best” evidence to help clinicians in making decisions about the care of individual patients in real-world practice.
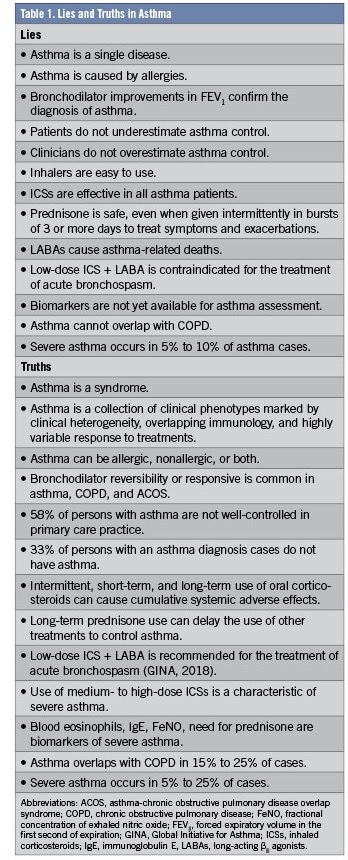
A frequent pitfall in clinical practice is to believe that guidelines are validated, but what if the collection of evidence creates a statistical entity that does not exist in real-world clinical practice? Who are we treating with guidelines? Is it the individual patient, or the statistical mean? Why is asthma today still as much a problem disease as it was in 1963? Where are the lies? (Table 1).
Among Mark Twain’s most famous quotes is, “Whenever you find yourself on the side of the majority, it is time to pause and reflect.” It is time to challenge the endorsements of guidelines by health insurance companies and governments, particularly in asthma, where using evidence-based protocols has not provided more-effective care with better outcomes or asthma control, which is still as unattainable as it was in 1963. The number of persons in the United States who reported 1 or more asthma attacks in 2015 exceeded 11 million, and the number of emergency department visits with the primary diagnosis of asthma reached 1.7 million.3
IS IT ASTHMA?
Asthma is not a single disease. Asthma is a syndrome or condition consisting of different phenotypes that present with nonspecific symptoms, marked by clinical heterogeneity, overlapping immunology, and highly variable response to drug therapy, all of which may account for the higher exacerbation rates and health care resource utilization for at least 5% to 25% of patients with asthma. Asthma should be a diagnosis of exclusion, since it shares clinical and pathophysiological features with chronic obstructive pulmonary disease (COPD) and asthma-COPD overlap syndrome (ACOS) (Figure 1).4

Establishing a diagnosis of asthma can no longer rely on detecting symptoms, which are all nonspecific (eg, wheezing, cough, dyspnea on exertion). It is a myth to believe that bronchodilator reversibility after albuterol treatment confirms the diagnosis of asthma when this is commonly found in COPD and ACOS.
The great irony today is that asthma is overdiagnosed by approximately 30%,5 but severe asthma, as described in recent guidelines, is underdiagnosed.6,7 It is a major pitfall to prescribe, refill, and forget about patients who cannot achieve asthma control after 3 months of treatment. Patients should be seen every 2 to 6 weeks until asthma control has been achieved (ie, Asthma Control Test [ACT] score ≥20). The burnout imposed by patient workloads, prior authorization, and electronic medical record-keeping can make “best practice” protocols camouflage for a hurriedly made diagnosis and treatment of asthma.8
SEVERE ASTHMA
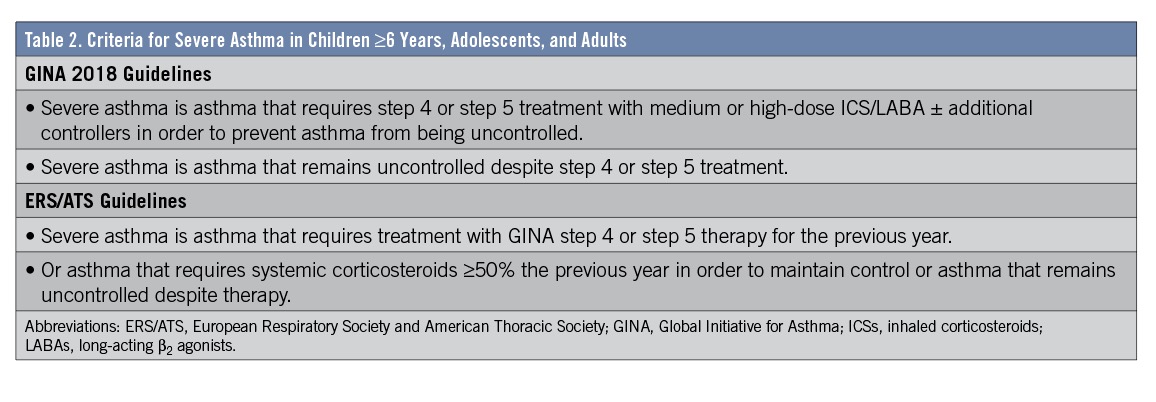
Severe asthma is defined as asthma that requires treatment with high-dose ICSs together with a second controller (and/or systemic corticosteroid) to prevent it from becoming “uncontrolled” despite this therapy.7 This definition includes patients who received an adequate trial of these therapies but whose treatment was stopped due to lack of response. (Table 2).
The lack of well-designed studies using a uniform definition of asthma means that available statistical data on the epidemiology of severe asthma are disparate, particularly in adults. Severe asthma varies in prevalence among countries (18% in Western Europe, 19% in the United States, and 32% in Central Europe), and approximately 50% of patients with severe asthma have poor disease control.9 Adult patients with uncontrolled asthma consume up to 85% of all health care dollars spent on asthma while representing 20% of all asthma patients.10
CONFUSION BY CONSENSUS
Asthma is capricious, prone to sudden and unaccountable changes in symptoms and control. The 2007 NIH-NAEPP guidelines and Expert Panel Report (EPR)2 leave clinicians with the impression that asthma is intermittent or persistent, and if persistent, it can be classified as mild, moderate, or severe depending on the patient’s need for albuterol, nocturnal awakening, and forced expiratory volume in the first second of expiration (FEV1) % predicted.
The NAEPP EPR severity classification scheme categorizes patients on characteristics that are present before the initiation of asthma controller therapy—ie, not previously treated with an ICS or an ICS plus a long-acting β2 agonist (LABA). Based on pretreatment asthma severity, preferred and alternative drug treatments are recommended. The NAEPP EPR labels of asthma severity—mild persistent, moderate persistent, and severe persistent pretreatment—are still employed in the ICD-10 codes.
The Global Initiative for Asthma (GINA) 2018 guidelines6 recommend assessing asthma severity retrospectively based on the level of treatment needed to control symptoms and prevent exacerbation, typically during a 3-month period of management (Table 3). The GINA labels of asthma control—mild, moderate, and severe—are based on whether the patient’s symptoms are well-controlled posttreatment. The mixup as to which label to use in clinical practice occurs daily and impacts patient treatment and asthma management. The NAEPP EPR report views asthma as a static disease with static severity, whereas GINA guidelines view asthma from the perspective of asthma control.

Using the GINA 2018 guidelines and the European Respiratory Society and American Thoracic Society (ERS/ATS) guidelines for severe asthma in clinical practice requires an understanding of the definition of asthma control. Asthma control is defined as the degree to which the observable effects of asthma can be seen in the patient or have been reduced by treatments retrospectively.6,7
The confusion from consensus guidelines is not obvious at first. Severe asthma can occur in patients with NIH-NAEPP–defined mild persistent, moderate persistent, or severe persistent asthma if they subsequently fail to control their symptoms and experience exacerbations with drug treatment, or if they required prednisone for 6 months or longer in the previous year. For example, a patient with moderate persistent asthma as defined by NAEPP EPR can develop severe asthma as defined by GINA. It is important to adopt GINA guidelines into clinical practice, not NAEPP EPR, and target asthma control, not asthma severity, when prescribing and stepping up or stepping down controller drug therapy.
The level of asthma control—whether well controlled, not well controlled, or very poorly controlled—can be determined by the Rules of Two characteristics based on the occurrence rate of daytime symptoms more than twice a week, the need for albuterol rescue more than twice a week, and nighttime awakening due to asthma twice or more monthly.6,7,11 A more objective measure of asthma control can be achieved using the ACT.
ASTHMA CONTROL TEST
The ACT (https://www.asthmacontroltest.com) is a validated questionnaire that is invaluable in assessing impairment in our patients at UC Davis, although it is limited by its 4-week self-assessment period and a sensitivity and specificity of 71% and 71%, respectively. An ACT score of less than 20 not only indicates uncontrolled asthma, but also is a criterion for severe asthma.12,13
It is a common pitfall to disregard the objective assessment of asthma control initially and at every clinic visit with clinical interview and the ACT. The minimally important difference of the ACT is 3, which is the smallest difference in score that would indicate that either a clinically important improvement or a worsening of asthma control has occurred.14 Uncontrolled asthma is very prevalent and exceeds 50% in adult patients despite the use of evidence-based guidelines.15,16
Guidelines for the management of asthma should never be used to impose a standard of care. They provide the basis for rational decisions in the management of severe and milder asthma cases. Clinicians, asthmatologists, third-party payers (including government and health insurance companies), and the courts should never view these recommendations as rules. To recall the wisdom of Dr Frazier, each asthma patient is an individual, and rules change with individuals.1 It is vital to conduct a clinical trial of one in every patient, one drug at a time.
At UC Davis, our approach during consultation is to first confirm the diagnosis, then determine the phenotype and subphenotype, and then conduct a clinical trial of one or treatment trial and error for each patient.10 The failure to control asthma by the patient and clinician after a period of 3 to 4 months should raise suspicion that the diagnosis of asthma is incorrect, or that an untreated comorbidity exists, or that severe asthma is present.
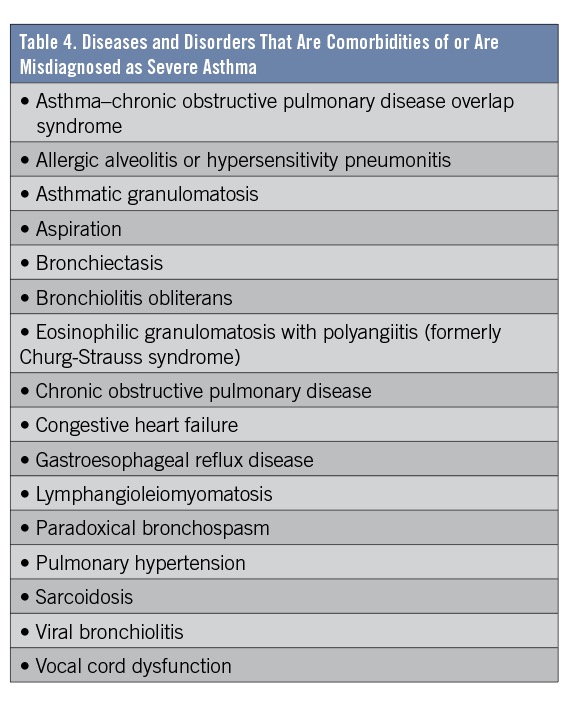
Confirm the diagnosis. All patients with asthma should be evaluated for the role of allergens as contributing factors to symptoms and acute exacerbations. Table 4 lists several findings supporting the concept that asthma is an exceedingly complex immunologic syndrome punctuated by clinical heterogeneity and highly variable responses to controller drug treatments.
Determine phenotype and subphenotype. Phenotype is based on whether the patient is allergic or nonallergic with asthma. Subphenotype is based on the presence or absence of eosinophilia (eosinophil count ≥150 cells/µL). Eosinophilic asthma is not always allergic asthma.
Sputum is underutilized as a biomarker of airway inflammation. Sputum analysis in asthmatics suggests the existence of 4 distinct subphenotypes: eosinophilic, neutrophilic, mixed, and paucigranulocytic asthma. The response to treatment traditionally aimed at Th2-high asthma is highly variable and could be recognized by the nonresponsiveness of a patient’s asthma control to inhaled or oral corticosteroids. The upregulation of specific cytokines creates profiles or patterns that may help direct clinical research and drug development to treat refractory asthma.17
Conduct a clinical trial of one. The patient-provider relationship is extremely important. Patients should be the driving force in asthma care. Outrageous as it sounds, this approach challenges the notion that the clinician controls asthma, not the patient. Only the patient can tell us whether asthma has been controlled (ie, ACT score of 20 or above in the absence of reliable biomarkers). A trinity between the patient, primary care provider, and asthmatologist must thrive. The patient cannot be the lesser party in the pursuit of asthma control.10 The primary care provider is often the asthmatologist when consultation with an allergist or pulmonologist is not possible. I am convinced by decades of clinical trials of one and trial and error that dynamic patient participation, whether with inhaler device training, or teaching what asthma control looks and feels like, hastens the achievement of personal asthma control.
Our experience at UC Davis has taught us that virtually every patient needs more disease-state education, inhaler device training, safety awareness, and a written asthma action plan to fully participate in the quest to control asthma. Each patient is told that their response to controller drug therapy can direct changes in treatment and management to individualize their care.
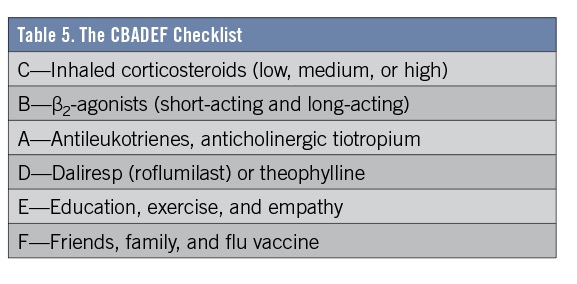
Instead of using the ABCDEF checklist described in a previous “Pulmonary Pitfalls” article on acute COPD exacerbations,18 use the CBADEF checklist, reversing the first 3 letters, to help clinicians and patients recall the action plan targeting more comprehensive care. (Table 5).
In primary care practice, we recommend a short-term, 6-week clinical trial of one with an ICS before adding a LABA, similar to that of the Predicting Response to Inhaled Corticosteroid Efficacy (PRICE) study protocol,19 which phenotyped ICS-naive asthmatics using the biomarkers FEV1, bronchodilator response, sputum eosinophils, fractional concentration of exhaled nitric oxide (FeNO), total immunoglobulin E (IgE), and negative methacholine challenge test results (PC20, the provocative concentration causing a 20% or more decrease in FEV1). Characteristics evaluated included length of asthma history, age, sex, height, weight, and ethnicity.
The objective of PRICE was to predict a patient’s response to short-term ICS treatment administered for 6 weeks. After responders and nonresponders to ICS treatment were identified, the second objective was then to evaluate whether a short-term response, or a lack of response, to an ICS can predict long-term asthma control. FEV1 response to ICS at the end of 6 weeks were either responders (identified as those with a greater than 5% improvement) or nonresponders (identified as those with a 5% or less change from baseline FEV1). Participants were then randomly assigned to a double-blind, placebo-controlled 16-week trial of either ICS or placebo to evaluate asthma control using the Asthma Control Questionnaire.
Many clinicians were alarmed to learn that 54% of participants were determined to be responders to ICS treatment, and 46% were categorized as nonresponders. The responders had a significantly lower FEV1% predicted and FEV1/forced vital capacity (FVC) ratio at baseline than the nonresponders.
What about the biomarkers popularly recommended by guidelines and recent articles in the literature? In PRICE, sputum eosinophils (1.7% in responders vs 1.1% in nonresponders), FeNO (15.4 ppm in responders vs 13.0 ppm in nonresponders), and total IgE were not statistically different between the 2 groups. Phenotyping was not helpful. In the subsequent 16-week placebo-controlled trial, responders lost asthma control on placebo while responders on ICSs maintained control, whereas nonresponders achieved the same level of asthma control on placebo as they did on ICSs. The need to conduct a clinical trial of one, one drug at a time, protects patients from unnecessary and avoidable treatments that will not improve asthma control.20
Patients with allergic (Th2-high) asthma manifest features of adaptive immunity and generally improve asthma control with ICSs, oral corticosteroids, antileukotriene drugs, prostaglandin D2 receptor blockers, anti-IgE therapy, and monoclonal antibodies against specific interleukins (eg, IL-5) or their receptors (IL-5 receptor blockers that cause antibody-redirected, cell-mediated, cytotoxic depletion of eosinophils by natural killer cells).20
Patients with nonallergic (Th2-low) asthma manifest features of innate immunity and typically do not improve asthma control with ICSs. This group of patients should be evaluated for biomarkers of eosinophilic, neutrophilic, mixed, or paucigranulocytic asthma (eg, in sputum counts or blood eosinophil counts). Persons with Th2-low asthma typically have increased sputum neutrophils or a paucigranulocytic profile, where the white blood cell count is not increased, and bronchial smooth muscle and airway neurons may be more important. Emerging evidence suggests that viral infection, obesity, and air pollution activate innate immunity mechanisms, and these Th2-low patients may not respond favorably to ICSs or oral corticosteroids.21 It is not science fiction to suggest that a patient with difficult-to-control asthma can have both adaptive and innate immune mechanisms, depending on the interaction of the patient with external triggers (eg, allergens, viruses, tobacco smoke, air pollution).
IS ASTHMA CONTROLLED?
Has asthma been controlled or not controlled for the past 3 months on treatment? Severe asthma is uncontrolled asthma defined as the presence of at least 1 of the following:
- Poor symptom control: ACT score <20
- Frequent severe exacerbations: 2 or more bursts of systemic corticosteroids in the previous year
- Serious exacerbations: at least 1 hospitalization, intensive care unit stay, or mechanical ventilation in the previous year
- Airflow limitation: reduced FEV1/FVC <0.70
- Controlled asthma that worsens on tapering of these high doses of ICSs or systemic corticosteroids (or additional biologics)
Before stepping up asthma treatment to high-dose ICS plus a LABA plus a long-acting muscarinic antagonist or biologic, consider all reasonable alternative diagnoses (Table 4). Common comorbidities that can accompany and aggravate asthma control are rhinosinusitis, gastroesophageal reflux disease, vocal cord dysfunction, pulmonary aspiration, obstructive sleep apnea, and heart failure.

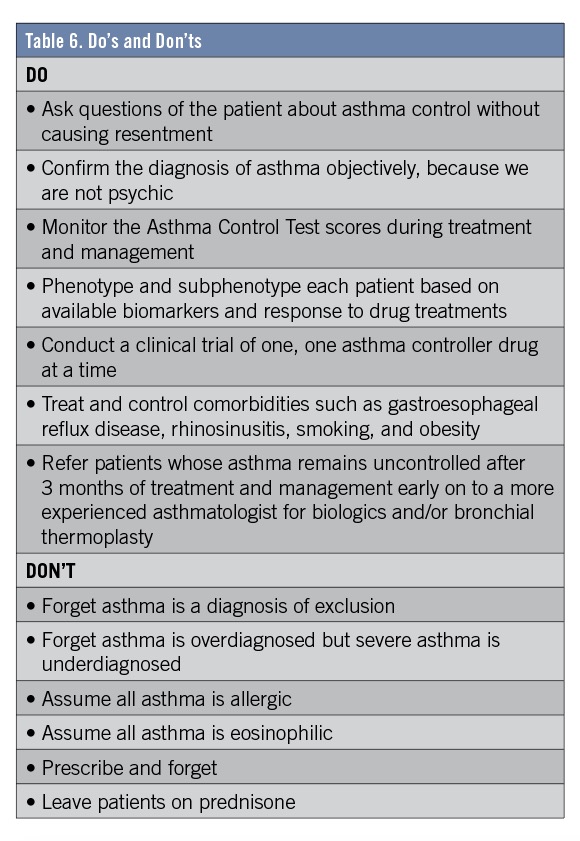
Consultation with a more experienced asthmatologist should be sought if the patient fails to achieve asthma control and/or has frequent exacerbations despite multiple controller treatments (Figure 2) and after review of the updated do’s and don’ts in Table 6.

CONSULTATION
There are many key aspects of consultation at UC Davis for severe asthma. First, we engage the patient to ascertain their understanding of and opinion about their asthma, including what has worked and what has not worked. We augment their education quickly on the goals of management to reduce impairment and to reduce risks from exacerbations and drug therapy before confronting the question of confirming the diagnosis and adherence to a written asthma action plan. The patient takes the Asthma Control Test, and the results are discussed with the patient. We attempt to phenotype the patient’s asthma clinically as allergic (Th2-high) or nonallergic (Th2-low), eosinophilic or noneosinophilic, and order tests if phenotyping has been incomplete. Spirometry, flow-volume loops, diffusing capacity for carbon monoxide (if available), and chest radiographs are reviewed. We ascertain the patient’s competency using his or her prescribed albuterol rescue inhaler and controller medications. Atrocious inhaler technique is to be expected.
The CBADEF tool is employed to explain the rationale for a clinical trial of one, and smoking status is explored, since smoking can render patients less-sensitive to ICSs and oral corticosteroids or raise the possibility of ACOS. Asthma control is assessed using the ACT every 4 weeks for 3 to 4 months. Only if asthma remains uncontrolled, or the presentation is atypical, or if the patient reports excessive mucus production, do we consider ordering chest computed tomography scan. Radiographic findings may reveal bronchiectasis, emphysema, or interstitial lung disease, which can accompany asthma concurrently. Bronchoscopy with bronchial biopsies and bronchoalveolar lavage is recommended if asthma remains uncontrolled. Clinical suspicion for allergic alveolitis (hypersensitivity pneumonitis), sarcoidosis, bronchiolitis obliterans, lymphangioleiomyomatosis, asthmatic granulomatosis, or Churg-Strauss syndrome may require video-assisted thoracotomy with lung biopsy for definitive diagnosis.
I cannot do better than to conclude with Dr Frazier’s 1963 remarks: “Asthma is a problem disease; its capricious nature defies control and keeps the health of the asthmatic always in a precarious state. And, improper treatment can make the asthma worse. Each person is an individual and rules change with individuals.”1
REFERENCES:
- Frazier CA. Treating allergic asthma: some do’s and don’ts. Consultant. 1963;3(7):24-26.
- Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma: Full Report 2007. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. https://www.nhlbi.nih.gov/sites/default/files/media/docs/asthgdln_1.pdf. Published August 28, 2007. Accessed November 30, 2018.
- Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats: Asthma. https://www.cdc.gov/nchs/fastats/asthma.htm. Updated March 21, 2017. Accessed November 30, 2018.
- Louie S, Zeki AA, Schivo M, et al. The asthma-chronic obstructive pulmonary disease overlap syndrome: pharmacotherapeutic considerations. Expert Rev Clin Pharmacol. 2013;6(2):197-219.
- Aaron SD, Vandemheen KL, FitzGerald JM, et al; Canadian Respiratory Research Network. Reevaluation of diagnosis in adults with physician-diagnosed asthma. JAMA. 2017;317(3):269-279.
- Global Strategy for Asthma Management and Prevention. Global Initiative for Asthma. https://ginasthma.org/2018-gina-report-global-strategy-for-asthma-management-and-prevention/. Revised March 29, 2018. Accessed November 30, 2018.
- Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343-373.
- Lemaire JB, Wallace JE. Burnout among doctors. BMJ. 2017;358:j3360.
- Rabe KF, Adachi M, Lai CK, et al. Worldwide severity and control of asthma in children and adults: the global Asthma Insights and Reality surveys. J Allergy Clin Immunol. 2004;114(1):40-47.
- Mealey FH, Kenyon NJ, Avdalovic MC, Louie S. Difficult-to-control asthma in adults. Am J Med. 2007;120(9):760-763.
- Millard M, Hart M, Barnes S. Validation of Rules of Two™️ as a paradigm for assessing asthma control. Proc (Bayl Univ Med Cent). 2014;27(2):79-82.
- Nathan RA, Sorkness CA, Kosinski M, et al. Development of the Asthma Control Test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59-65.
- Schatz M, Sorkness CA, Li JT, et al. Asthma Control Test: reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J Allergy Clin Immunol. 2006;117(3):549-556.
- Schatz M, Kosinski M, Yarlas AS, Hanlon J, Watson ME, Jhingran P. The minimally important difference of the Asthma Control Test. J Allergy Clin Immunol. 2009;124(4):719-723e.1.
- Mintz M, Gilsenan AW, Bui CL, et al. Assessment of asthma control in primary care. Curr Med Res Opin. 2009;25(10):2523-2531.
- Peters SP, Jones CA, Haselkorn T, Mink DR, Valacer DJ, Weiss ST. Real-world Evaluation of Asthma Control and Treatment (REACT): findings from a national Web-based survey. J Allergy Clin Immunol. 2007;119(6):1454-1461.
- Green RH, Brightling CE, Bradding P. The reclassification of asthma based on subphenotypes. Curr Opin Allergy Clin Immunol. 2007;7(1):43-50.
- Craddock KM, Lipe C, Vukovich CM, et al. Acute exacerbations of COPD: avoiding danger and death. Consultant. 2016;56(8):740-744.
- Martin RJ, Szefler SJ, King TS, et al; National Heart, Lung, and Blood Institute’s Asthma Clinical Research Center. The Predicting Response to Inhaled Corticosteroid Efficacy (PRICE) trial. J Allergy Clin Immunol. 2007;119(1):73-80.
- Stokes JR, Casale TB. Characterization of asthma endotypes: implications for therapy. Ann Allergy Asthma Immunol. 2016;117(2):121-125.
- Fitzpatrick AM, Moore WC. Severe asthma phenotypes—how should they guide evaluation and treatment? J Allergy Clin Immunol Pract. 2017;5(4):901-908.