
Peer Reviewed
A Girl With an Asymptomatic Mass on Her Eyelid
Answer: Chalazion

A chalazion, meaning “hailstone” in Greek, is a localized lipogranulomatous inflammation that affects the meibomian gland of the eyelid.1,2 The condition is also known as meibomian cyst. It is the most common inflammatory lesion of the eyelid and typically presents as a painless localized swelling on the eyelid.1
INCIDENCE
Chalazion is one of the most common eyelid disorders of all age groups.2,3 The exact incidence, however, is not known. The male to female ratio is approximately equal.4 Adio and colleagues reviewed the records of children seen over 1 year in the eye clinic of the University of Port Harcourt Teaching Hospital in Nigeria.4 A total of 846 children were seen. The male to female ratio was 1 to 1.07. Most patients were between 13 and 18 years of age. Four (0.47%) of the 846 had a diagnosed chalazion.
ETIOPATHOGENESIS
There are approximately 30 meibomian glands in the upper eyelid and 10 to 20 meibomian glands in the lower eyelid.5,6 Meibomian glands consist of holocrine branching tubuloalveolar modified sebaceous glands, unconnected with hair or erector pili muscle, and are arranged vertically on the posterior surface of the tarsus.5,7 A chalazion results from blockage of the meibomian gland by desquamated epithelial cells and/or lipid inspissation.5,7 Rupture of the meibomian gland with release of the inspissated lipid into the surrounding tissue elicits a granulomatous inflammatory reaction.6,7 Since meibomian glands are embedded in the tarsal plate of the eyelids, a chalazion due to blockage of the meibomian gland results in a mass on the conjunctival portion of the eyelid.8
The etiology is multifactorial, including local and systemic inflammatory conditions. Factors predisposing to blockage of meibomian glands include poor lid hygiene, meibomian gland dysfunction, chronic blepharitis, seborrheic dermatitis, rosacea, vitamin A deficiency, Demodex brevis infestation, viral keratitis (adenovirus, Epstein-Barr virus, herpes simplex virus), pulmonary tuberculosis, hyperimmunoglobulin E syndrome, smoking, and bortezomib therapy.9-23
HISTOPATHOLOGY
Histopathologically, there is often a connective tissue pseudocapsule surrounding a lipogranulomatous lesion with lipid-filled, Touton-type giant cells.1,8 Characteristically, the nuclei of these cells are located around a central foamy cytoplasmic area that contains the lipid material.8
CLINICAL MANIFESTATIONS
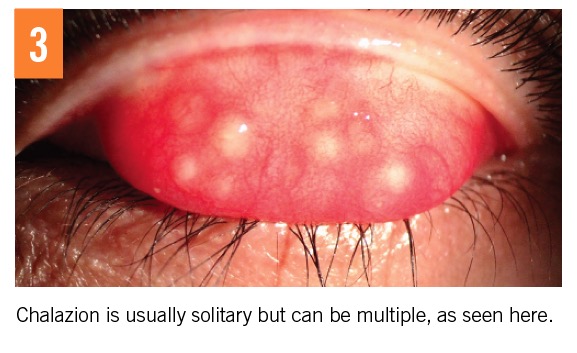
Clinically, a chalazion presents with a firm, nontender, slowly growing, nodule on the upper or lower eyelid.24 The upper eyelid is more commonly involved due to the increased number and length of meibomian glands in the upper eyelid.6,25 The lesion is usually less than 1 cm in diameter.8 A chalazion may occur externally as a lump on the skin, as illustrated in the present case, or internally as a lump beneath the conjunctiva (Figure 2).24 The condition is usually solitary but can be multiple (Figure 3).
A chalazion is usually painless and nonerythematous.24,26,27 A small chalazion may not be visible but is palpable as a mass or resistant area in the tarsus. Extratarsal presentation of chalazion has also been described, resulting from anterior perforation of the tarsal plate with inferior migration of meibomian gland secretions, resulting in a reddish intradermal nodule on the lower eyelid skin.28,29
DIAGNOSIS
The diagnosis is mainly clinical. Typically, a chalazion presents as a nontender, nonerythematous, slowly growing nodule on the eyelid with no evidence of inflammation, no punctum, and no discharge. Laboratory tests are usually not necessary.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis includes, among others, hordeolum, cellulitis, idiopathic facial aseptic granuloma, epidermoid cyst, dermatofibroma, neurofibroma, pilomatrixoma, blue nevus, external angular dermoid, lipoma, milium, pneumo-orbita, pyogenic granuloma, seborrheic keratosis, sebaceous gland hyperplasia, amyloidosis, and neoplasms.1
A hordeolum is an acute infection of the eyelid that is usually staphylococcal in origin. When it involves the gland of Zeis (sebaceous) or Moll (sweat), it is termed an external hordeolum, commonly referred to as a stye.30 Less commonly, the meibomian gland on the inner side of the eyelid can become infected, and it is termed an internal hordeolum. Characteristically, an external hordeolum presents as a painful, yellowish pustule in the eyelid margin, typically centered on an eyelash with surrounding erythema (Figure 4).
An internal hordeolum, on the other hand, presents as a tender swelling within the tarsal plate.30 The lesion may resolve into a chalazion. A chalazion can be differentiated from a hordeolum by the absence of signs of acute inflammation. In contrast with a hordeolum, a chalazion is painless.10
Cellulitis of the eyelid can be distinguished from a chalazion by diffuse swelling, erythema, and significant pain. The condition may be accompanied by fever and leukocytosis.
An idiopathic facial aseptic granuloma typically presents as a painless, erythematous to violaceous, soft nodule on the eyelid or cheek.31-33 The lesion usually resolves spontaneously without scarring over several months to a year.31
An epidermoid cyst, also known as epidermal inclusion cyst or epidermal cyst, typically presents as an asymptomatic, solitary, fluctuant to firm, dome-shaped mass that is attached to the skin but not attached to the underlying structure.34-36 A punctum is often noted.35 It has a tendency to grow slowly. Epidermoid cysts occur mainly on hair-bearing areas and often result from the trauma to the pilosebaceous unit.36 In non–hair-bearing areas, epidermoid cysts result from implantation and proliferation of squamous epithelium into the dermis secondary to trauma.36 Sites of predilection include the face, scalp, neck, and back.34-36
A dermatofibroma is a common benign dermal lesion composed primarily of fibroblasts with excessive deposition of collagen in the dermis. The condition most frequently affects young adults and occasionally children and is more common in females than in males.37 Typically, the lesion presents as an asymptomatic red or reddish brown nodule.37,38 The lesion is attached to the skin but not to the underlying structure. Although the lesion can develop anywhere on the body, the lesion is most commonly found on the limb. The size varies from a few millimeters to 2 cm. Pinching of the lesion results in dimpling of the lesion (the dimple sign or Fitzpatrick sign).38,39 This can be attributed to tethering of the epidermis to the underlying lesion.
A neurofibroma is a benign peripheral nerve-sheath tumor composed of an extracellular matrix and a heterogeneous mixture of Schwann cells and fibroblasts.40 Cutaneous neurofibromas often appear during puberty or pregnancy and increase in size and number with age and are found in almost all adults with neurofibromatosis type 1. These painless, flesh-colored, soft or elastic, nodular or pedunculated lesions often invaginate into the skin and exhibit the buttonhole sign when gentle digital pressure is applied to the surface. In contrast, subcutaneous neurofibromas, which are usually firm and painful, are deeply seated in the dermis and therefore are less circumscribed.40 A solitary neurofibroma on the eyelid may simulate a chalazion.41-43
Typically, a pilomatrixoma presents as a firm to hard, solitary, painless nodule in the dermis or subcutaneous tissue covered by normal skin. The color varies from white, pink, blue, to red-blue.44 Most lesions measure 0.5 cm to 3 cm in diameter. The nodule may become hardened if the lesion is calcified. Calcification and ossification occurs in 70% to 85% and 15% to 20% of patients, respectively.45 Downward pressure directed at one end of the lesion may cause the other end to spring upward in the skin (teeter-totter sign).45 Multiple facets and angles may appear when the overlying skin is stretched (tent sign).45 An eyelid pilomatrixoma may masquerade as a chalazion.46 In one study, more than 75% of cases of eyelid pilomatrixoma occurred in patients younger than 13 years of age.47
A common blue nevus typically presents as a solitary, smooth, well-circumscribed, dome-shaped papule or nodule that measures less than 1 cm in diameter.48,49 The lesion is homogeneously blue to blue-gray to blue-black in color and is asymptomatic. The characteristic blue color can be attributed to the deep dermal location of melanin and that shorter-wavelength blue light cannot penetrate deeply but is reflected back to the observer (Tyndall effect).48 It is commonly located on the face and dorsal surfaces of the hands and feet.49
An external angular dermoid is a dermoid cyst located at the lateral orbital rim adjacent to the frontozygomatic suture.50 The cyst arises along bony sutures as a result of abnormal ectodermal sequestration during embryonic development. Clinically, an external angular dermoid presents as an asymptomatic, slow-growing, soft to firm, poorly mobile mass above the lateral eyebrow.25 The mass is subcutaneous, and the overlying skin is normal. The mass is usually noticed at birth or in the first year of life.
A lipoma is a benign tumor composed of collections of mature adipocytes enclosed by a thin, fibrous capsule. Clinically, a lipoma presents as an asymptomatic, slow-growing, soft, well-circumscribed, lobulated, round or oval, dome-shaped or egg-shaped mass that is not attached to the overlying skin or underlying structures.51 The overlying skin is characteristically normal. A “slipping sign,” elicited by gently sliding the fingers off the edge of the tumor, is characteristic.51 The tumor will be felt to slip out from under. The size of a lipoma usually ranges from 2 to 5 cm in diameter. Although rare, a lipoma can occur on the eyelid.
A milium is a benign, 1- to 2-mm, white or yellowish, dome-shaped, superficial keratinous cyst.52,53 Histologically, a milium appears as a small infundibular cyst that is lined with stratified squamous epithelium with a granular cell layer.53 The cyst contains laminated layers of keratin. The lesion is most common on the face.52
A pneumo-orbita often results from facial trauma leading to airflow between the sinuses and the orbit.54 Clinically, a pneumo-orbita presents with an acute onset of ocular pain, edema, and hyperemia of the eyelid, exacerbated by expiratory movements such as sneezing and coughing.54
A pyogenic granuloma, also known as lobular capillary hemangioma, is a common, acquired, benign vascular proliferation of the skin and mucous membrane. Clinically, a pyogenic granuloma presents as an asymptomatic soft, dome-shaped papule/nodule or a sessile or pedunculated papule/nodule with a smooth, glistening, erosive, or friable surface.55,56 The color is usually bright red to purple to dusky red initially because of the high number of blood vessels. With time, the vascularity decreases, and the lesion tends to become more collagenized and pink.56
Characteristically, seborrheic keratosis presents as an asymptomatic, sharply demarcated, round or oval plaque with a “stuck on” warty appearance. It is typically brown but may be yellow, reddish, or black.57,58 Often, the lesion appears oily and shiny, hence the misnomer “seborrheic” (greasy) keratosis. The face is a site of predilection.
Sebaceous hyperplasia is an asymptomatic common and benign proliferation of sebaceous glands. The condition usually presents as a solitary, or more commonly, as multiple discrete, yellow or flesh-colored, dome-shaped papules.59,60 Individual lesions are usually 2 to 5 mm in diameter. The face is most commonly affected.59
Amyloidosis is characterized by abnormal extracellular accumulation and deposition of amyloid fibrils.61 Cutaneous amyloid deposits may occur with both primary or systemic amyloidosis.62 Primary cutaneous amyloidosis of the eyelid, especially if unilateral, may masquerade as a chalazion.61,62
Benign tumors (eg, trichilemmal cyst, keratinous cyst, pleomorphic adenoma, sebaceoma, leiomyoma)63-67 and malignant tumors (eg, sebaceous carcinoma, squamous cell carcinoma, basal cell carcinoma, Meckel cell carcinoma, lymphoma, plasmacytoma)68-76 involving the eyelid may mimic a chalazion.
Miscellaneous conditions that may masquerade as a chalazion include retained soft contact lens, lacrimal gland duct stone, para-canalicular abscess, and tuberculosis of the eyelid.50,77-80
COMPLICATIONS
A chalazion may be cosmetically unsightly.81 The lesion may become secondarily infected. Rarely, an infected lesion may lead to preseptal cellulitis, especially in an atopic individual.27 At times, the lesion may rupture and result in the formation of pyogenic granuloma. A chalazion may be associated with meibomian gland dysfunction or chronic blepharitis.25,82 If the lesion is large enough, it may cause visual problems such as astigmatism, decreased vision, and hyperopia by exerting pressure on the eyeball.3,10,15,25,80 Recurrence of chalazion is common.
PROGNOSIS
Without treatment, up to 25% of cases may resolve spontaneously within 6 months.83 Some untreated cases may take several years to resolve.84
MANAGEMENT
Up to 80% of chalazia resolve with conservative treatment consisting of eyelid hygiene, twice daily warm compresses for 10 to 15 minutes, and gentle lid massage.6,7,10,25,81,82 Warm compresses help to soften the plug of material so that it is easier to drain.6 The massage should be performed over the lesion, in the direction of the eyelashes to promote drainage of the obstructed gland.7,25 Topical antibiotic should be used if the lesion is infected.7 If the chalazion fails to resolve with conservative treatment and is cosmetically blemishing, a surgical approach should be considered.
Intralesional corticosteroid injection is a therapeutic option for the treatment of chalazion.7,85 The procedure can be painful.85 On the other hand, subcutaneous corticosteroid injection into the looser extralesional tissue results in less pain.85 Because skin depigmentation may occur at the injection site, subconjunctival corticosteroid injection rather than subcutaneous corticosteroid injection is preferred, especially in patients with a darker complexion.3 Large lesions or lesions that fail to respond to 2 or 3 corticosteroid injections may require subconjunctival incision and curettage.2,5,26 Anterior orbital cyst formation may occur as a late complication of surgery for chalazion.86 A meta-analysis of 8 randomized control trials comparing incision and curettage (n = 264) with intralesional corticosteroid injections (n = 288) showed that incision and curettage was more effective than intralesional corticosteroid injections, with a success rate of 78% vs 60.4%, respectively.87 Combination of incision and curettage with corticosteroid injections is more comfortable for patients and can achieve a success rate of approximately 98%.88-90



REFERENCES:
- Özdal PÇ, Codère F, Callejo S, Caissie AL, Burnier MN. Accuracy of the clinical diagnosis of chalazion. Eye. 2004;18(2):135-138.
- Unal M. Chalazion treatment. Orbit. 2008;27(6):397-398.
- Ben Simon GJ, Huang L, Nakra T, Schwarcz RM, McCann JD, Goldberg RA. Intralesional triamcinolone acetonide injection for primary and recurrent chalazia: is it really effective. Ophthalmology. 2005;112(5):913-917.
- Adio AO, Alikor A, Awoyesuku E. Survey of pediatric ophthalmic diagnoses in a teaching hospital in Nigeria. Niger J Med. 2011;20(1):105-108.
- Dhaliwal U, Bhatia A. A rationale for therapeutic decision-making in chalazia. Orbit. 2005;24(4):227-230.
- Lederman C, Miller M. Hordeola and chalazia. Pediatr Rev. 1999;20(8):283-284.
- Gilchrist H, Lee G. Management of chalazia in general practice. Aust Fam Physician. 2009;38(5):311-314.
- Jordan GA, Beier K. Chalazion. StatPearls. https://www.statpearls.com/as/eyes/19276/. Updated May 18, 2018. Accessed November 14, 2018.
- Aoki M, Kawana S. Bilateral chalazia of the lower eyelids associated with pulmonary tuberculosis. Acta Derm Venereol. 2002;82(5):386-387.
- Arbabi EM, Kelly RJ, Carrim ZI. Chalazion. BMJ. 2010;341:c4044.
- Chen L, Chen X, Xiang Q, et al. Prevalence of low serum vitamin A levels in young children with chalazia in southwest China. Am J Ophthalmol. 2014;157(5):1103-1108.e2.
- Crama N, Toolens AMP, van der Meer JWM, Cruysberg JRM. Giant chalazia in the hyperimmunoglobulinemia E (hyper-IgE) syndrome. Eur J Ophthalmol. 2004;14(3):258-260.
- Fraunfelder FW, Yang HK. Association between bortezomib therapy and eyelid chalazia. JAMA Ophthalmol. 2016;134(1):88-90.
- Grob SR, Jakobiec FA, Rashid A, Yoon MK. Chalazia associated with bortezomib therapy for multiple myeloma. Ophthalmology. 2014;121(9):1845-1847.e3.
- Jin KW, Shin YJ, Hyon JY. Effects of chalazia on corneal astigmatism: large-sized chalazia in middle upper eyelids compress the cornea and induce the corneal astigmatism. BMC Ophthalmol. 2017;17(1):36.
- Laaribi N, Abdellaoui T, Abaloun Y, et al. Chalazia associated with bortezomib therapy. J Fr Ophtalmol. 2018;41(8):e381-e382.
- Liang L, Ding X, Tseng SCG. High prevalence of Demodex brevis infestation in chalazia. Am J Ophthalmol. 2014;157(2):342-348.e1.
- Malekahmadi M, Farrahi F, Tajdini A. Serum vitamin A levels in patients with chalazion. Med Hypothesis Discov Innov Ophthalmol. 2017;6(3):63-66.
- Nemet AY, Vinker S, Kaiserman I. Associated morbidity of chalazia. Cornea. 2011;30(12):1376-1381.
- Patteri P, Serru A, Chessa ML, Loi M, Pinna A. Recurrent giant chalazia in hyperimmunoglobulin E (Job’s) syndrome. Int Ophthalmol. 2009;29(5):415-417.
- Schear MJ, Milman T, Steiner T, Shih C, Udell IJ, Steiner A. The association of Demodex with chalazia: A histopathologic study of the eyelid. Ophthalmic Plast Reconstr Surg. 2016;32(4):275-278.
- Yam JCS, Tang BSF, Chan T-M, Cheng ACK. Ocular demodicidosis as a risk factor of adult recurrent chalazion. Eur J Ophthalmol. 2014;24(2):159-163.
- Yin Y, Gong L. The evaluation of meibomian gland function, morphology and related medical history in Asian adult blepharokeratoconjunctivitis patients. Acta Ophthalmol. 2017;95(6):634-638.
- Leung AKC. Chalazion. In: Leung AKC, ed. Common Problems in Ambulatory Pediatrics: Specific Clinical Problems. Vol 2. New York, NY: Nova Science Publishers; 2011:107-110.
- Leung AKC. Lumps and bumps in children: cysts. Consultant Pediatricians. 2012;11(5):134-136.
- Duarte AF, Moreira E, Nogueira A, Santos P, Azevedo F. Chalazion surgery: advantages of a subconjunctival approach. J Cosmet Laser Ther. 2009;11(3):154-156.
- Dubey R, Wang LW, Figueira EC, et al. Management of marginal chalazia: a surgical approach. Br J Ophthalmol. 2011;95(4):590,596-597.
- Chang M, Park J, Kyung SE. Extratarsal presentation of chalazion. Int Ophthalmol. 2017;37(6):1365-1367.
- Korekawa A, Nakajima K, Makita E, Nakano H, Sawamura D. External chalazion as reddish and intractable lower eyelid nodules in a child. J Dermatol. 2017;44(5):e93-e94.
- McAlinden C, González-Andrades M, Skiadaresi E. Hordeolum: acute abscess within an eyelid sebaceous gland. Cleve Clin J Med. 2016;83(5):332-334.
- Borok J, Holmes R, Dohil M. Idiopathic facial aseptic granuloma—a diagnostic challenge in pediatric dermatology. Pediatr Dermatol. 2018;35(4):490-493.
- Ozer PA, Gurkan A, Kurtul BE, Kabatas EU, Beken S. Comparative clinical outcomes of pediatric patients presenting with eyelid nodules of idiopathic facial aseptic granuloma, hordeola, and chalazia. J Pediatr Ophthalmol Strabismus. 2016;53(4):206-211.
- Zitelli KB, Sheil AT, Fleck R, Schwentker A, Lucky AW. Idiopathic facial aseptic granuloma: review of an evolving clinical entity. Pediatr Dermatol. 2015;32(4):e136-e139.
- Kang S-G, Kim C-H, Cho H-K, Park M-Y, Lee Y-J, Cho M-K. Two cases of giant epidermal cyst occurring in the neck. Ann Dermatol. 2011;23(suppl 1):S135-S138.
- Leung AKC, Barankin B. A ruptured erythematous mass on a teen’s cheek. Consultant Pediatricians. 2013;12(12):541-543.
- Nigam JS, Bharti JN, Nair V, et al. Epidermal cysts: a clinicopathological analysis with emphasis on unusual findings. Int J Trichology. 2017;9(3):108-112.
- Leung AKC, Barankin B. Dermatofibroma. Consultant. 2016;56(6):560-561.
- Sampaio FMS, Gualberto GV, Cerqueira FGMd, Cerqueira AMMd, Treu CM, Vargas TJdS. Case for diagnosis. An Bras Dermatol. 2014;89(3):519-520.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, de Daniel-Rodríguez C, Jiménez-Gómez N, Ballester-Martínez A. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14(2):98-101.
- Leung AKC, Barankin B, Leung AAM. What are this woman’s widespread asymptomatic nodules? Consultant. 2017;57(11):651-654.
- Chen N, Hsu Y-H, Lee Y-C. Solitary neurofibroma of eyelid masquerading as chalazion. Int Med Case Rep J. 2017;10:177-179.
- Pai HV, Abbagani S, Jaishankar PP. Isolated neurofibroma of the eyelid mimicking recurrent chalazion. Indian J Ophthalmol. 2018;66(3):451-453.
- Shibata N, Kitagawa K, Noda M, Sasaki H. Solitary neurofibroma without neurofibromatosis in the superior tarsal plate simulating a chalazion. Graefes Arch Clin Exp Ophthalmol. 2012;250(2):309-310.
- Lee S-Y, Ryu Y-J, Her Y, Sung K-Y. Pilomatricoma: an unusual presentation. Ann Dermatol. 2014;26(6):791-792.
- Leung AKC, Fong JHS. Pilomatricoma. Consultant Pediatricians. 2004;3(3):142.
- Hada M, Meel R, Kashyap S, Jose C. Eyelid pilomatrixoma masquerading as chalazion. Can J Ophthalmol. 2017;52(2):e62-e64.
- Levy J, Ilsar M, Deckel Y, Maly A, Anteby I, Pe’er J. Eyelid pilomatrixoma: a description of 16 cases and a review of the literature. Surv Ophthalmol. 2008;53(5):526-535.
- Leung AKC, Barankin B. An adolescent with a smooth, blue-black nodule on the dorsal wrist. Consultant Pediatricians. 2014;13(11):501-503.
- Murata T, Kaku Y, Morita K. Common blue nevus on the upper lip: a case report. J Dermatol. 2012;39(4):419-420.
- Agrawal V, Acharya H, Agarwal P, Sekhon V, Sharma D. Subcutaneoscopic excision of external angular dermoid cyst in children without conspicuous scarring. Asian J Endosc Surg. 2013(3):241-244.
- Leung AKC, Barankin B. Lipoma. Consultant. 2017;57(5):317-318.
- Kansal NK, Agarwal S. Neonatal milia. Indian Pediatr. 2015;52(8):723-724.
- Leung AKC, Barankin B. Benign primary milia. Consultant Pediatricians. 2014;13(4):191-192.
- Marzuillo P, Aliberti F, Tipo V. Pneumo-orbita mimicking hordeolum. Arch Dis Child. 2016;101(2):183.
- Leung AKC, Barankin B. Pyogenic granuloma. Consultant. 2017;57(4):248-250.
- Ting PT, Barankin B. Pyogenic granuloma. Can Fam Physician. 2006;52:35-36.
- Karadag AS, Parish LC. The status of the seborrheic keratosis. Clin Dermatol. 2018;36(2):275-277.
- Leung AKC, Leung AAC. Seborrheic keratosis. Consultant. 2012;52(8):573-575.
- Leung AKC, Barankin B. What are these asymptomatic papules on a man’s cheeks and forehead? Consultant. 2017;57(6):355-357.
- Wang Q, Liu J-M, Zhang Y-Z. Premature sebaceous hyperplasia in an adolescent boy. Pediatr Dermatol. 2011;28(2):198-200.
- Manaa Alkatan H, Al-Mohizea A, Alsuhaibani A. A case of localized amyloidosis of the eyelid misdiagnosed as recurrent chalazion. Saudi J Ophthalmol. 2017;31(3):180-182.
- Nair AG, Mukherjee B, Krishnakumar S, Biswas J, Mehta RA. Unilateral primary cutaneous amyloidosis of the eyelid masquerading as a chalazion. Can J Ophthalmol. 2014;49(5):e112-e114.
- Ahuja S, Rao VA, Kumar P, Rajesh N, Srinivasan R. Sebaceoma of the conjunctiva presenting as a chalazion. Indian J Dermatol. 2014;59(5):521-522.
- Hui JI, Buchser NM, Dubovy SR. Primary eyelid leiomyoma. Ophthalmic Plast Reconstr Surg. 2011;27(4):e102-e103.
- Jordan D, Stoica B, Brownstein S, Ali-Ridha A. Intratarsal keratinous cyst mimicking a large chalazion. Can J Ophthalmol. 2014;49(6):e149-e151.
- Meena M, Mittal R, Saha D. Trichilemmal cyst of the eyelid: masquerading as recurrent chalazion. Case Rep Ophthalmol Med. 2012;2012:261414.
- Wang Y, Maltry A, Mokhtarzadeh A. Pleomorphic adenoma of an accessory lacrimal gland masquerading as a chalazion. Ophthalmology. 2017;124(7):952.
- Al-Mujaini A, Sabt B, Al-Hadabi I. It is not chalazion. Oman J Ophthalmol. 2013;6(1):63-69.
- Fuente García C, Pinilla-Pagnon I, Albandea Jiménez A, Sales-Sanz M. Sebaceous carcinoma mimicking a chalazion in a young patient. Arch Soc Esp Oftalmol. 2018;93(8):e56-e57.
- Gill M, Garg S, Kalra R, Sen R. Sebaceous carcinoma of the eyelid diagnosed on fine needle aspiration cytology. J Cytol. 2012;29(1):75-76.
- Nemoto Y, Arita R, Mizota A, Sasajima Y. Differentiation between chalazion and sebaceous carcinoma by noninvasive meibography. Clin Ophthalmol. 2014;8:1869-1875.
- Maheshwari R, Maheshwari S. Extramedullary pasmacytoma masquerading as chalazion. Orbit. 2009;28(2-3):191-193.
- Makrygiannis G, Vahdani K, Giasin O. Muir-Torre syndrome masquerading as chalazion. Ophthalmic Plast Reconstr Surg. 2015;31(5):422-423.
- Miguel AIM, Salgado MB, Lisboa MS, Henriques F, Paiva MC, Castela GPL. Pediatric ocular rosacea: 2 cases. Eur J Ophthalmol. 2012;22(4):664-666.
- Sagili S, Malhotra R. The importance of considering sebaceous gland carcinoma in presumed chalazia in South Asian patients? Br J Gen Pract. 2013;63(607):74.
- Waisbourd M, Leibovitch I, Sayar D, Elhasid R. Conjunctival lymphoma in a child. Cornea. 2011;30(5):598-599.
- Almaliotis D, Nakos E, Siempis T, et al. A para-canalicular abscess resembling an inflamed chalazion. Case Rep Ophthalmol Med. 2013;2013:618367.
- Kim SC, Lee K, Lee SU. Lacrimal gland duct stones: misdiagnosed as chalazion in 3 cases. Can J Ophthalmol. 2014;49(1):102-105.
- Mittal R, Tripathy D, Sharma S, Balne PK. Tuberculosis of eyelid presenting as a chalazion. Ophthalmology. 2013;120(5):1103, 1103.e3-1103.e4.
- Agarwal PK, Ahmed TY, Diaper CJM. Retained soft contact lens masquerading as a chalazion: a case report. Indian J Ophthalmol. 2013;61(2):80-81.
- Wu AY, Gervasio KA, Gergoudis KN, Wei C, Oestreicher JH, Harvey JT. Conservative therapy for chalazia: is it really effective? Acta Ophthalmol. 2018;96(4):e503-e509.
- Mansour AM, Chan C-C, Crawford MA, et al. Virus-induced chalazion. Eye. 2006;20(2):242-246.
- Cottrell DG, Bosanquet RC, Fawcett IM. Chalazions: the frequency of spontaneous resolution. Br Med J (Clin Res Ed). 1983;287(6405):1595.
- Honda M, Honda K. Spontaneous resolution of chalazion after 3 to 5 years. Eye Contact Lens. 2010;36(4):230-232.
- Chung CF, Lai JSM, Li PSH. Subcutaneous extralesional triamcinolone acetonide injection versus conservative management in the treatment of chalazion. Hong Kong Med J. 2006;12(4):278-281.
- Alsuhaibani AH, Al-Faky YH. Large anterior orbital cyst as a late complication of chalazion surgical drainage. Eye (Lond). 2015;29(4):585-587.
- Aycinena AR, Achiron A, Paul M, Burgansky-Eliash Z. Incision and curettage versus steroid injection for the treatment of chalazia: A meta-analysis. Ophthalmic Plast Reconstr Surg. 2016;32(3):220-224.
- Biuk D, Matić S, Barać J, Vuković MJ, Biuk E, Matić M. Chalazion management—surgical treatment versus triamcinolon application. Coll Antropol. 2013;37(suppl 1):247-250.
- Epstein GA, Putterman AM. Combined excision and drainage with intralesional corticosteroid injection in the treatment of chronic chalazia. Arch Ophthalmol. 1988;106(4):514-516.
- Putterman AM. Re: “incision and curettage versus steroid injection for treatment of chalazia: a meta-analysis.” Ophthalmic Plast Reconstr Surg. 2017;33(2):151.