
Peer Reviewed
Leclercia adecarboxylata Osteomyelitis of the Leg With Infected Hardware in an Immunocompetent Patient
Authors:
Chinelo Animalu, MD, MPH
Assistant Professor, College of Medicine, Department of Medicine, Division of Infectious Diseases, University of Tennessee Health Science Center, Memphis, Tennessee
Adam Carrera, MD
Resident, College of Medicine, University of Tennessee Health Science Center, Memphis, Tennessee
Shirin Mazumder, MD
Associate Professor, College of Medicine, Department of Medicine, Division of Infectious Diseases, University of Tennessee Health Science Center, Memphis, Tennessee
Citation:
Animalu C, Carrera A, Mazumder S. Leclercia adecarboxylata osteomyelitis of the leg with infected hardware in an immunocompetent patient [published online August 6, 2019]. Infectious Diseases Consultant.
A previously healthy 44-year-old man accidentally fell from a deer stand while hunting and sustained multiple orthopedic injuries, including a left femur fracture, a left pilon fracture, an L3 vertebral compression fracture, an L1-L3 transverse process fracture, and bilateral first and second rib fractures. He underwent left femur nailing and fixation of left pilon fracture.
Following the operations, he initially had been doing well, but approximately 2 months later, during a routine visit at the wound care center, was noted to have some wound dehiscence on the distal incision site on the lateral left lower extremity. He was treated empirically with a 1-month course of cephalexin in the outpatient orthopedic clinic; however, progressive wound dehiscence was noted. His only complaint was some discomfort along the surgical site. He denied any associated fever, chills, nausea, vomiting, aches, and pain. Based on the progression of the wound, a decision was made to admit him to the hospital for further management.
At the time of his initial presentation to the hospital, he was afebrile and hemodynamically stable. His vital signs included the following: temperature, 37.2°C; blood pressure, 138/90 mm Hg; pulse 85 beats/min; respiratory rate, 20 breaths/min; and oxygen saturation, 100% on room air.
Laboratory findings showed the following: blood urea nitrogen, 12 mg/dL; creatinine, 1.03 mg/dL; white blood cell count, 8700/µL; hemoglobin, 12.1 g/dL; hematocrit, 36.7%; platelets, 326 × 103/µL; erythrocyte sedimentation rate, elevated at 25 mm/h; and C-reactive protein, elevated at 6.66 mg/L.
A radiograph of the left tibia and fibula showed postoperative changes of the distal tibia and fibula with stabilization plates and orthopedic screws. No evidence of acute fracture, dislocation, or subluxation was noted other than an acute-to-remote appearing fracture of the distal third of the fibula. He underwent surgical debridement and irrigation; at that time, the distal wound was probed and went directly down to the bone, with the distal plate communicating with this fresh wound dehiscence. A sequential debridement of all nonviable skin, muscle, fascia and subcutaneous tissues were done.
Gram stain of the surgical cultures showed lactose-fermenting gram-negative rods, and culture was positive for pansusceptible Leclercia adecarboxylata. Identification and antibiotic susceptibility testing was performed using the Microscan WalkAway SI 96 automated system (Figure). Confirmation was performed using MALDI-TOF mass spectrometry.
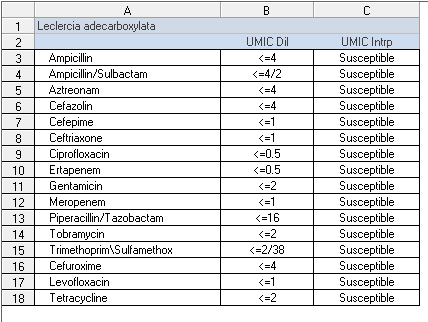
Figure. Antibiotic susceptibility report.
He completed a 6-week course of ertapenem through a peripherally inserted central line and subsequently underwent a continuous course of oral antibiotic suppression with minocycline, 100 mg, twice per day, given that he still had hardware in place. The patient did well on this regimen and did not have any further problems with the wound.
Discussion. Leclercia adecarboxylata is an aerobic, motile, gram-negative bacillus that belongs to the Enterobacteriaceae family. It was originally described in 1962 by Leclerc as Escherichia adecarboxylata,1 but it later was designated as Leclercia, since it could be phenotypically distinguished from other species of the Enterobacteriaceae family.2 It is found in a variety of foods, water, and animals such as snails and slugs. It has been isolated from human stool and is found to be part of normal gut flora of animals.3
Typically, L adecarboxylata infections are considered to be opportunistic and are found alone in immunosuppressed patients or as polymicrobial infections in immunocompetent patients.3-6 Cases have been reported, however, of L adecarboxylata infections in immunocompetent patients without coinfection.3-5
While L adecarboxylata infections are not commonly reported, the organism shares many characteristics with Escherichia coli, and this may point to misdiagnosis and underestimation of its impact on patient health. With advances in laboratory testing, L adecarboxylata can be more accurately isolated and distinguished from E coli than previously. For instance, unlike E coli, L adecarboxylata sometimes possess positivity for urease hydrolysis, grow in the presence of potassium cyanide, and utilize malonate; some strains produce yellow pigment. It also differs from E coli by the lack of lysine and ornithine decarboxylase and the inability to ferment d-sorbitol.3 Furthermore, additional techniques such as antimicrobial susceptibilities and mass spectrometry can expand current understanding of the clinical significance and prevalence of L adecarboxylata infections.5
In the case described here, dehiscence of the patient’s surgical wound communicated directly with surgical plating that was placed for stabilization of his pilon fracture. The mechanism by which the organism gained access to the site is unknown, but the hardware should be considered as a possible source, since cases of L adecarboxylata infection have been reported in association with foreign bodies and other medical devices (central venous lines).7 The patient was prescribed and completed a 1-month course of cephalexin, but his wound continued to worsen, requiring initiation of intravenous ertapenem for 6 weeks. As has been observed in the literature, this strain of L adecarboxylata was sensitive to all antimicrobials, although there have been documented instances of it producing extended-spectrum β-lactamase activity with resistance to ceftazidime, cefotaxime, aztreonam, and cefepime.3,8
Since 1991, approximately 24 documented cases have been reported in humans, with most being polymicrobial opportunistic infections ranging from catheter-related bacteremia to spontaneous bacterial peritonitis. A few cases have also been reported in immunocompetent individuals.9 This patient’s case describes the first documented incidence of L adecarboxylata being the causative organism of osteomyelitis in a human patient with or without immunocompromise. With the availability of more extensive laboratory evaluation in the identification of bacteria, documented isolation of L adecarboxylata as an infectious pathogen will likely increase and allow clinicians to more completely understand this organism’s role in human pathology and treat it more effectively.
References:
- Leclerc H. Biochemical study of pigmented Enterobacteriaceae [in French]. Ann Inst Pasteur (Paris). 1962;102:726-74
- Tamura K, Sakazaki R, Kosako Y, Yoshizaki E. Leclercia adecarboxylata gen. nov., comb. nov., formerly known as Escherichia adecarboxylata. Curr Microbiol. 1986;13(4):179-184.
- Bali R, Sharma P, Gupta K, Nagrath S. Pharyngeal and peritonsillar abscess due to Leclercia adecarboxylata in an immunocompetent patient. J Infect Dev Ctries. 2013;7(1):46-50.
- Anuradha M. Leclercia adecarboxylata isolation: case reports and review. J Clin Diagn Res. 2014;8(12):DD03-DD0
- Hess B, Burchett A, Huntington MK. Leclercia adecarboxylata in an immunocompetent patient. J Med Microbiol. 2008;57(pt 7):896-898.
- Daza RM, Iborra J, Alonso N, Vera I, Portero F, Mendaza P. Isolation of Leclercia adecarboxylata in a cirrhotic patient [in Spanish]. Enferm Infecc Microbiol Clin. 1993;11(1):53-54.
- Grantham WJ, Funk SS, Schoenecker JG. Leclercia adecarboxylata musculoskeletal infection in an immune competent pediatric patient: an emerging pathogen? Case Rep Orthop. 2015;2015:160473.
- Mazzariol A, Zuliani J, Fontana R, Cornaglia G. Isolation from blood culture of a Leclercia adecarboxylata strain producing an SHV-12 extended-spectrum beta-lactamase. J Clin Microbiol. 2003;41(4):1738-1739.
- Keren Y, Keshet D, Eidelman M, Geffen Y, Raz-Pasteur A, Hussein K. Is Leclercia adecarboxylata a new and unfamiliar marine pathogen? J Clin Microbiol. 2014;52(5):1775-1776.