
Peer Reviewed
What Caused This Older Man’s Persistent Desaturation?
Answer: A. Cryptogenic organizing pneumonia
Reassessment of the patient’s presentation and findings resulted in a differential diagnosis of cryptogenic organizing pneumonia (COP). The patient was given intravenous methylprednisolone, 1 mL/kg/d, and had significant improvement of his respiratory symptoms within 24 hours. Serial chest radiographs taken at follow-up demonstrated partial resolution of infiltrates compared with previous imaging studies (Figure 3).

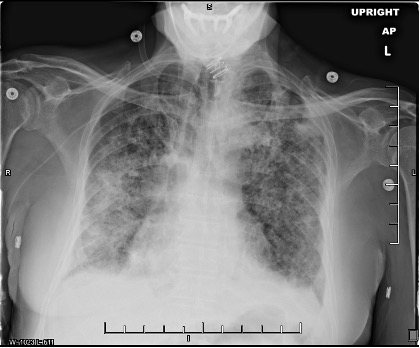
Figure 3. Chest radiographs taken 1 week (a, top) and 2 weeks (b, bottom) after initiating intravenous glucocorticoid therapy. The patient had been extubated and demonstrated significant improvement of symptoms during this period.Discussion. COP is a rare idiopathic interstitial lung disease that requires surgical biopsy for confirmation.1,2 In scenarios in which a biopsy is unavailable and the patient is intubated—such as in our case—careful consideration is needed. Adverse effects of glucocorticoids in a critically ill patient include immunosuppression and increased risk for potentially fatal nosocomial infection.3 Trial therapy should be started only if other, more common diagnoses have been excluded and if imaging studies are consistent with COP or another inflammatory process, such as acute respiratory distress syndrome. Fortunately, in our case, radiograph and CT findings did feature lower lobe consolidation and infiltration described in other reports of COP.3,4 Once suspicion for COP is high, the patient should be consulted on the risks of surgical lung biopsy vs trial glucocorticoid therapy and be offered a choice in which step to take next.
Diagnosis of COP can be delayed because of presentation overlap with other, more common forms of pneumonia (eg, CAP, idiopathic pulmonary fibrosis, chronic eosinophilic pneumonia).1,6 These delays can put patients at greater risk for progression to acute respiratory failure. Surgical lung biopsy for confirmation of COP may become unavailable in these situations. Our case serves to provide clinical experience for the diagnosis and treatment of COP in the acute care setting. The presentation, imaging studies, and treatment of our patient should improve the current archive and clinical detection and treatment of this rare disease in the future.
Patient outcome. Although the patient refused a lung biopsy to confirm COP, his presentation, imaging results, and rapid improvement in response to steroids were considered diagnostic for the condition. He was discharged home with long-term oral prednisone, ipratropium bromide/albuterol inhaler as needed, home oxygen, and pulsating vest. He has since made a full recovery and has not had any relapse of symptoms since therapy was completed; however, CT findings more than 1 year following his admission have demonstrated cylindrical bronchiectasis, scarring, and cystic changes secondary to inflammation because of the condition.
References
1. Cordier JF. Cryptogenic organising pneumonia. Eur Resp J. 2006;28(2):422-446. https://doi.org/10.1183/09031936.06.00013505
2. Colby TV. Pathologic aspects of bronchiolitis obliterans organizing pneumonia. Chest. 1992;102(suppl 1):38S-43S. https://doi.org/10.1378/chest.102.1_Supplement.38S
3. Drakopanagiotakis F, Polychronopoulos V, Judson MA. Organizing pneumonia. Am J Med Sci. 2008;335(1):34-39. https://doi.org/10.1097/MAJ.0b013e31815d829d
4. Müller NL, Staples CA, Miller RR. Bronchiolitis obliterans organizing pneumonia: CT features in 14 patients. Am J Roentgenol. 1990;154(5):983-987. https://doi.org/10.2214/ajr.154.5.2108572
5. Chang J, Han J, Kim DW, et al. Bronchiolitis obliterans organizing pneumonia: clinicopathologic review of a series of 45 Korean patients including rapidly progressive form. J Korean Med Sci. 2002;17(2):179-186. https://doi.org/10.3346/jkms.2002.17.2.179