
Peer Reviewed
Transient Erythroblastopenia of Childhood
AUTHORS:
Sukjoo Cho, MD1,2 • Lana Soylu, MD2
AFFILIATIONS:
1Hallym University College of Medicine, Chuncheon, South Korea
2University of South Florida Morsani College of Medicine, Tampa, Florida
CITATION:
Cho S, Soylu L. Transient erythroblastopenia of childhood. Consultant. 2020;60(7):e2. doi:10.25270/con.2020.05.00009
Received September 13, 2019. Accepted January 22, 2020.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Lana Soylu, MD, Associate Professor of Pediatrics, University of South Florida Health, 2 Tampa General Cir, 5th Floor, Tampa FL 33606 (lmccaule@usf.edu)
A 2-year-old previously healthy boy presented for a well-child visit. His diet consisted of a variety of fruits, vegetables, and meats, and he drank approximately 16 oz of whole milk per day and took a daily children’s multivitamin (not prescribed). His urine output and bowel movements were normal without diarrhea or hematochezia. His immunizations were up to date. His vital signs, growth and development, and physical examination findings were within normal limits.
The result of a routine screening test for hemoglobin was low at 8.0 g/dL, and his lead level was normal at less than 2 µg/dL. His previous hemoglobin test result 1 year ago had been in the normal range at 12.5 g/dL, and his newborn screening test results also had been normal.
His parents denied any bruising, bleeding, fever, night sweats, chills, decrease in activity level, bloody stools, or paleness in the boy, and they reported no recent illnesses. There was no family history of anemia or bleeding disorders.
A complete blood cell count (CBC), a reticulocyte count, and iron studies were ordered and revealed the following results: white blood cell (WBC) count, 8700/µL (reference range, 4000-12,000/µL) with elevated lymphocytes and an otherwise normal differential; hemoglobin, 8.0 g/dL (reference range, 11.5-14.5 g/dL); hematocrit, 25.3% (reference range, 33% to 43%); mean corpuscular volume (MCV), 82 µm3 (reference range, 76-90 µm3); mean corpuscular hemoglobin concentration, 31.6 g/dL (reference range, 32-36 g/dL); platelet count, 372 × 103/µL (reference range, 150-400 × 103/µL); reticulocytes, 6.6% (reference range, 0.5%-1.5%); total iron binding capacity, 319 µg/dL (reference range, 250-400 µg/dL); ferritin, 74 ng/mL (reference range, 10-60 ng/mL); and a normal hemoglobin electrophoresis result. Serum parvovirus B19 antibodies were not detected. The pathology review of his peripheral smear confirmed that the boy had a moderate normochromic, normocytic anemia with mild lymphocytosis.
A hemoglobin test was repeated after 10 days, the result of which was 10.3 g/dL with an MCV of 82 µm3 and a reticulocyte count of 5.0%. Given the patient’s anemia and elevated reticulocyte count, a consulting hematologist recommended checking lactate dehydrogenase and haptoglobin levels, which were found to be normal. The patient remained asymptomatic.
In light of the improving anemia and the normal iron studies results with the initial elevation in his reticulocyte count, he received a diagnosis of transient erythroblastopenia of childhood (TEC), which was already resolving. He was asked to follow up in 3 months to check his hemoglobin concentration, which at that time was found to be normal.
DISCUSSION
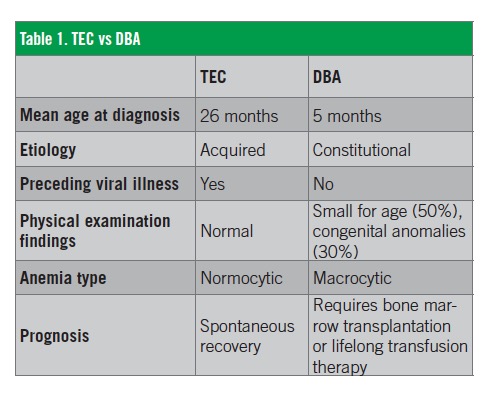
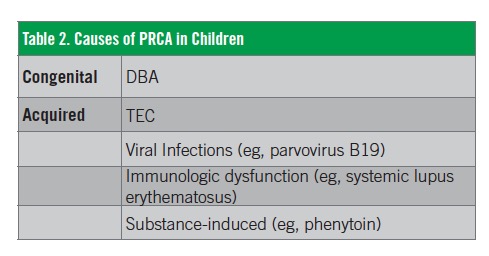
Pure red cell aplasia (PRCA) is a clinical syndrome characterized by decreased or absent erythroid precursor cells in an otherwise normocellular bone marrow.1 Patients with PRCA typically have an isolated anemia with reticulocytopenia.1 TEC is a benign, temporary, and acquired PRCA that was first described by Wranne in 1970, compared with a chronic and congenital Diamond-Blackfan anemia (DBA) (Table 1).2-4 Other causes of PRCA are listed in Table 2.4 TEC is an uncommon cause of PRCA in children and is likely subclinical in many cases.1 TEC should be suspected in a normocytic anemia with a low reticulocyte count in an otherwise healthy child.1,4
The pathophysiologic mechanism of TEC remains unclear.1,4 Based on the common association with a viral-like illness, a theory has been proposed that TEC is caused by virus-induced suppression of erythropoiesis.4 Parvovirus B19, echovirus 11, and human herpesvirus 6 have been hypothesized as possible causative agents,5-7 but no causal relationship has yet been established.1 Seasonal clustering, which can be a clue supporting the viral etiology theory, has been noted in some studies but denied in other studies.8-10 Some reports describing the occurrence of TEC in siblings suggest the possibility of an underlying genetic predisposition and unknown environmental triggers.11 To date, the involvement of no specific gene has been identified.4,11
It is difficult to differentiate the clinical manifestations of TEC from temporary PRCA caused by viral infections. Similar to TEC, certain viruses can suppress erythropoiesis without apparent anemia in normal children.1 Parvovirus B19 is the most common cause of such infection.4 However, the virus is more commonly associated with aplastic crisis in patients with hemolytic anemias such as sickle cell disease.1,4
TEC usually occurs in patients older than 6 months of age, particularly those between the ages of 1 and 4 years.1,3 Boys are affected slightly more often than girls.1,3 Most patients seek medical attention because of signs of severe anemia (eg, pallor, tiredness, anorexia).1 A history of a viral illness as indicated by symptoms of upper respiratory tract infection and diarrhea, is common 2 to 3 months before the development of TEC.1,3 Except for the signs of anemia, physical examination findings are mostly unremarkable.1
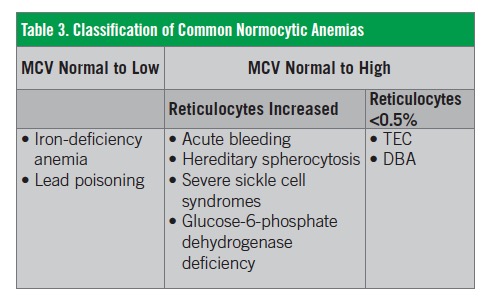
Children with TEC usually have normochromic, normocytic anemia, with an average hemoglobin concentration of 5.6 g/dL.4 The classification of common normocyte anemias is shown in Table 3.12 The reticulocyte count is usually below 1.0% but may be elevated, as in our patient’s case, if the patient is in the recovery stage.3,4 Although the MCV is generally within normal limits, it may be temporarily increased during the recovery stage due to reticulocytosis.1,3 WBC and platelet counts are typically in the normal range.4 The serum iron level is often found to be elevated, which reflects the decreased utilization of iron secondary to impaired erythrocytosis.3 Results of a direct Coombs test are negative.3 Serum ferritin, vitamin B12, and folate levels are normal.1
Most children with TEC undergo a spontaneous recovery within 1 to 2 months after diagnosis.4 Symptomatic cases may require red blood cell transfusion.1 No other treatments, including corticosteroids and intravenous immunoglobulin, have been proven to accelerate recovery.1,3 Recurrence is rare.4
SUMMARY
TEC is a benign condition characterized by normocytic anemia with reticulocytopenia of unknown etiology. It is most often subclinical and completely resolves without treatment after 1 to 2 months. Initial evaluation of TEC should focus on other possible causes of anemia, including DBA.5 Understanding its clinical and laboratory features will equip the physician to offer appropriate reassurance to parents and avoid unnecessary workup and therapy.3
REFERENCES:
- van den Akker M, Dror Y, Odame I. Transient erythroblastopenia of childhood is an underdiagnosed and self-limiting disease. Acta Paediatr. 2014;103(7):e288-e294. doi:10.1111/apa.12634
- Wranne L. Transient erythroblastopenia in infancy and childhood. Scand J Haematol. 1970;7(2):76-81. doi:10.1111/j.1600-0609.1970.tb01872.x
- Oski FA. Transient erythroblastopenia. Pediatr Rev. 1982;4(1):25-27. doi:10.1542/pir.4-1-25
- Perkins SL. Pediatric red cell disorders and pure red cell aplasia. Am J Clin Pathol. 2004;122 suppl:S70-S86. doi:10.1309/3WWXLGK5U2MC0X9B
- Wodzinski MA, Lilleyman JS. Transient erythroblastopenia of childhood due to human parvovirus B19 infection. Br J Haematol. 1989;73(1):127-128. doi:10.1111/j.1365-2141.1989.tb00231.x
- Elian JC, Frappaz D, Pozzetto B, Freycon F. Transient erythroblastopenia of childhood presenting with echovirus 11 infection. Acta Paediatr. 1993;82(5):492-494. doi:10.1111/j.1651-2227.1993.tb12731.x
- Penchansky L, Jordan JA. Transient erythroblastopenia of childhood associated with human herpesvirus type 6, variant B. Am J Clin Pathol. 1997;108(2):127-132. doi:10.1093/ajcp/108.2.127
- Cherrick I, Karayalcin G, Lanzkowsky P. Transient erythroblastopenia of childhood: prospective study of fifty patients. Am J Pediatr Hematol Oncol. 1994;16(4):320-324.
- Skeppner G, Kreuger A, Elinder G. Transient erythroblastopenia of childhood: prospective study of 10 patients with special reference to viral infections. J Pediatr Hematol Oncol. 2002;24(4):294-298. doi:10.1097/00043426-200205000-00015
- Burns RA, Woodward GA. Transient erythroblastopenia of childhood: a review for the pediatric emergency medicine physician. Pediatr Emerg Care. 2019;35(3):237-240. doi:10.1097/PEC.0000000000001760
- Shaw J, Meeder R. Transient erythroblastopenia of childhood in siblings: case report and review of the literature. J Pediatr Hematol Oncol. 2007;29(9):659-660. doi:10.1097/MPH.0b013e31814684e9
- Segel GB, Hirsh MG, Feig SA. Managing anemia in pediatric office practice: part 1. Pediatr Rev. 2002;23(3):75-84. doi:10.1542/pir.23-3-75