
Peer Reviewed
Portal Hypertension–Induced Varices in a Well-Appearing Child
AUTHORS:
Matthew Baker, MD, and Christopher Kuo, MD
Children’s Hospital Los Angeles, Los Angeles, California
CITATION:
Baker M, Kuo C. Portal hypertension–induced varices in a well-appearing child [published online January 7, 2020]. Consultant360.
A 2-year-old girl with a history of hematemesis presented to the emergency department after an episode of hematemesis composed of bright red blood mixed with large blood clots. The girl had been in her normal state of health and had been found covered in bloody emesis on the morning of presentation, but without pain or distress.
The parents denied any ingestions or trauma, and findings of the review of systems and family history were otherwise negative. Of note, the girl had been admitted to an outside hospital for observation after an episode of hematemesis 4 months prior to this presentation. Her hospital course had been unremarkable, and she received a diagnosis of anemia and a recommendation for a gastroenterology specialty follow-up visit; however, she had been lost to follow-up due to a lack of health insurance.
On presentation at the current visit, the girl was tachycardic (heart rate, 131 beats/min) with otherwise normal vital signs. Physical examination findings were notable for splenomegaly. She was anemic (hemoglobin, 7.4 g/dL) and thrombocytopenic (platelet count, 71 × 103/µL), but she had otherwise normal chemistry panel and liver function test results.
She received a blood transfusion and underwent abdominal ultrasonography, the results of which provided limited information due to the patient’s intolerance. Esophagogastroduodenoscopy (EGD) revealed large esophageal and gastric varices (Figure 1), two of which displayed signs of recent bleeding warranting sclerotherapy and banding. She was then placed on an octreotide infusion while awaiting further workup.

Figure 1. Large tortuous varices (grade 3) were noted on ultrasonography, extending from the junction of the upper and middle esophagus to the distal esophagus, two with stigmata of recent bleeding (red wale sign).
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for pediatric hematemesis is broad and includes etiologies such as foreign body trauma, a Mallory-Weiss tear, esophagitis or gastritis, ulcers, an arterial bleed such as a Dieulafoy lesion, epistaxis, and emesis of a red-colored solution. The urgent assessment of clinical stability when a child presents with hematemesis is crucial and should be followed by a thorough history and physical examination and a focused workup to unveil the source of the bleed. A child presenting specifically with the triad of hematemesis, splenomegaly, and thrombocytopenia is indicative of varices, a byproduct of portal hypertension (PHT), and warrants subsequent evaluation.
PHT can be cirrhotic or noncirrhotic and is defined by increased venous pressure gradients at different locations in the portal venous system.1-3 Cirrhotic PHT in pediatric patients is often a comorbidity associated with diseases resulting in hepatocellular injury, such as viral or autoimmune hepatitis, cystic fibrosis, biliary atresia, and Wilson disease.1,4 Noncirrhotic PHT occurs as a result of obstruction that is nonhepatocellular and can be the result of many underlying pathologies, including thrombosis, malignancy, infections, and disease processes causing severe splenomegaly.1,2,5,6 Schistosomiasis, which results in PHT due to parasitic eggs causing blockage of portal venules, is one of the leading causes of noncirrhotic PHT worldwide.7 However, in this healthy, well-appearing child, there were no clinical clues suggesting an underlying cause of her PHT.
DIAGNOSIS AND PATIENT COURSE
The patient underwent extensive workup for her suspected PHT. Computed tomography angiography (CTA) of the abdomen showed multiple small collateral vessels in the porta hepatis, compatible with cavernous transformation with absence of the portal vein (Figure 2).
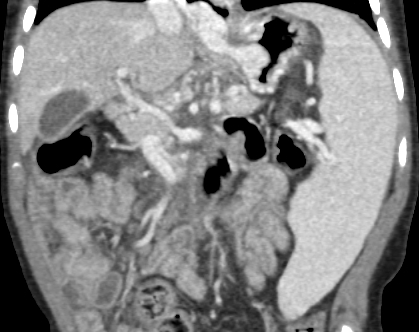
Figure 2. Multiple small collateral vessels in the porta hepatis, compatible with cavernous transformation with absence of portal vein.
An interventional radiologist performed a retrograde portogram, which also offered poor visualization of the main portal vein as a result of cavernous transformation secondary to portal vein thrombosis (PVT).
Due to the association of inherited thrombophilias or coagulopathies with PVT, an extensive hematologic workup was pursued without any abnormal findings. She subsequently underwent surgical shunt placement with a splenoadrenal-renal shunt to correct the PHT. She was placed on prophylactic fondaparinux for 4 weeks following shunt placement to prevent thrombosis of the shunt, but she was cleared by a hematologist after that time without a clear underlying cause of her PVT. The patient underwent a repeated EGD 1 month after shunt placement, the results of which showed marked improvement of her esophageal varices without any jaundice, icterus, melena, hematemesis, or abdominal pain.
TREATMENT
Pediatric PVT is estimated to occur in 1.3 of 100,000 live births, but this is likely an underestimation, since most are discovered incidentally or in cases where progression to PHT has occurred.8 One of the most common risk factors is umbilical venous catheter (UVC) placement, which is further influenced by the duration of the UVC and the catheter tip location and transfusion usage.8,9 Other known risk factors include omphalitis and neonatal sepsis.10
More than 50% of cases of PVT in the pediatric population are of an unknown etiology.8,10 Although PVT is not common in the pediatric age group, it is attributed as the cause of up to 20% of cases of PHT in children and is one of the main morbidities in upper gastrointestinal (GI) tract bleeds. Thus, it is pertinent that the management of PHT in the setting of PVT focus on treatment of varices to prevent upper GI bleeding. This includes acute treatment options such as β-adrenergic antagonists vs banding and sclerotherapy, or longer-term management options such as surgical shunt placement.8
TAKE-HOME MESSAGE
• PHT-induced varices must be considered in any child presenting with the triad of hematemesis, splenomegaly, and thrombocytopenia.
• PHT can be cirrhotic or noncirrhotic, which precludes clinicians from being able to rule out PHT in the setting of normal hepatic imaging and laboratory workup results.
• Most (>50%) cases of PVT in children do not have an identifiable cause.
• Treatment of PVT in pediatric patients should focus on preventing upper GI varices and bleeding.
REFERENCES:
- Intagliata NM, Caldwell SH, Tripodi A. Diagnosis, development, and treatment of portal vein thrombosis in patients with and without cirrhosis. Gastroenterology. 2019;156(6):1582-1599.e doi:10.1053/j.gastro.2019.0265
- Khanna R, Sarin SK. Idiopathic portal hypertension and extrahepatic portal venous obstruction. Hepatol Int. 2018;12(suppl 1):148-167. doi:10.1007/s12072-018-9844-3
- Sarin SK, Khanna R. Non-cirrhotic portal hypertension. Clin Liver Dis. 2014;18(2):451-476. doi:10.1016/j.cld.2014.01.009
- Gonzalez RS, Washington K. Pediatric liver disease. In: Gonzalez RS, Washington K. Non-Neoplastic Liver Pathology: A Pathologist’s Survival Guide. Basel, Switzerland: Springer International Publishing Switzerland; 2016:chap 15.
- Trebicka J, Strassburg CP. Etiology and complications of portal vein thrombosis. Viszeralmedizin. 2014;30(6):375-380. doi:10.1159/000369987
- Schouten JN, Garcia-Pagan JC, Valla DC, Janssen HL. Idiopathic noncirrhotic portal hypertension. Hepatology. 2011;54(3):1071-1081. doi:10.1002/hep.24422
- Dunn MA, Kamel R. Hepatic schistosomiasis. Hepatology. 1981;1(6):653-661. doi:10.1002/hep.1840010615
- Kumar R, Kerlin BA. Thrombosis of the abdominal veins in childhood. Front Pediatr. 2017;5:18 doi:10.3389/fped.2017.00188
- Morag I, Epelman M, Daneman A, et al. Portal vein thrombosis in the neonate: risk factors, course, and outcome. J Pediatr. 2006;148(6):735-73 doi:10.1016/j.jpeds.2006.01.051
- Ferri PM, Ferreira AR, Fagundes EDT, Liu SM, Roquete MLV, Penna FJ. Portal vein thrombosis in children and adolescents: 20 years experience of a pediatric hepatology reference center. Arq Gastroenterol. 2012;49(1):69-76. doi:1590/s0004-28032012000100012