
Peer Reviewed
An Atlas of Lumps and Bumps: Part 6
AUTHORS:
Alexander K. C. Leung, MD1,2 —Series Editor • Benjamin Barankin, MD3 • Joseph M. Lam, MD4 • Kin Fon Leong, MD5
AFFILIATIONS:
1Department of Pediatrics, University of Calgary, Calgary, Alberta, Canada
2Alberta Children’s Hospital, Calgary, Alberta, Canada
3Toronto Dermatology Centre, Toronto, Ontario, Canada
4Department of Pediatrics and Department of Dermatology and Skin Sciences, University of British Columbia, Vancouver, British Columbia, Canada
5Pediatric Institute, Kuala Lumpur General Hospital, Kuala Lumpur, Malaysia
CITATION:
Leung AKC, Barankin B, Lam JM, Leong KF. An atlas of lumps and bumps, part 6. Consultant. 2021;61(7):e16-e18. doi:10.25270/con.2021.06.00008
DISCLOSURES:
Dr Leung is the series editor. He was not involved with the handling of this paper, which was sent out for independent external peer review.
CORRESPONDENCE:
Alexander K. C. Leung, MD, #200, 233 16th Ave NW, Calgary, AB T2M 0H5, Canada (aleung@ucalgary.ca)
EDITOR’S NOTE:
This article is part of a series describing and differentiating dermatologic lumps and bumps. To access previously published articles in the series, visit https://bit.ly/35J1I1v.
Molluscum Contagiosum
Molluscum contagiosum is a common cutaneous infectious disease caused by a poxvirus of the molluscipox genus in the Poxviridae family.1-4 The prevalence is approximately 7% of immunocompetent children.5 This condition is most common in children 2 to 5 years of age but is also common in sexually active teenagers and young adults.1-4,6 Molluscum contagiosum is rare in infants.7 The male to female ratio is approximately equal.8 The virus is transmitted mainly by close physical contact with infected skin, followed by autoinoculation and, occasionally, by contaminated fomites.4 Predisposing factors include poor hygiene, poverty, overcrowding, atopic dermatitis, and immunodeficiency.1,4
Typically, molluscum contagiosum presents as discrete, smooth, firm, waxy, dome-shaped papules with characteristic central dell or umbilication (Figures 1 and 2) from which a plug of cheesy material, which contains virus particles and dead epithelial cells, can be expressed.2-4,9 Central umbilication can be hard to observe in young children and small lesions.4,9 Dermoscopy aids visualization of the central umbilication, which may not be obvious to the naked eye. Dermoscopy shows a central umbilication with well-defined polylobular, roundish or 4-leaved clover-like, white to yellowish amorphous structures surrounded by a peripheral crown of reddish, linear, or branched vessels (Figure 3). The color of the lesions can be translucent, flesh-colored, pearly white, yellow, pink or red (especially when irritated or inflamed).4,10 The lesions are most common in areas of skin rubbing or moist regions.11 In children, the most commonly affected areas are the extremities (Figure 4), trunk, intertriginous areas, and genitals (Figure 5).12 Lesions on the genital areas can be mistaken for penile warts (Figure 5). In adults, particularly those who are sexually active, lesions are more common on the lower abdomen, upper thighs, pubic area, and anogenital area.1,4,12 Atypical locations include lips,13 oral mucosa,14 areolae,15 nipples,15 eyelids,16 conjunctiva,17 scalp,18 and soles.12,19

Figure 1.
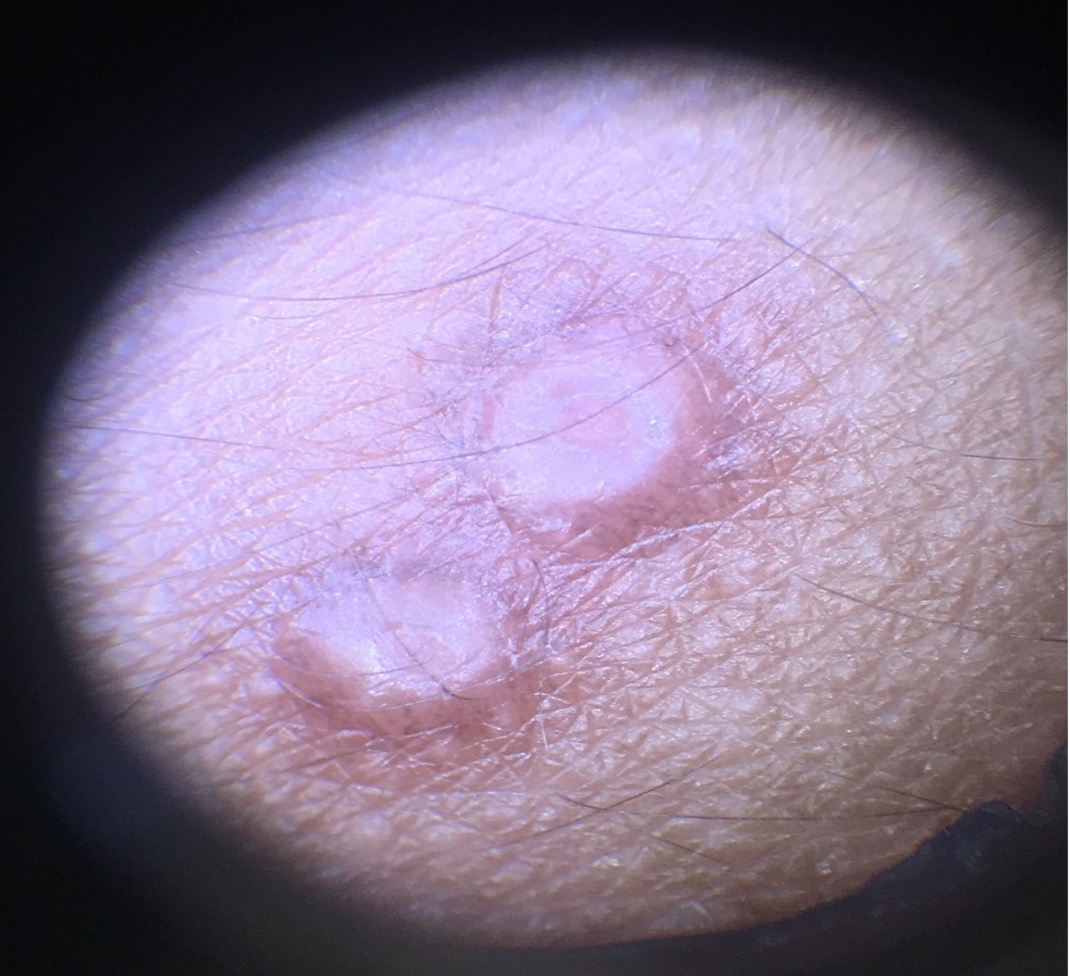
Figure 2.

Figure 3.

Figure 4.

Figure 5.
In general, the size of lesions ranges from 1 to 5 mm in diameter (Figure 6), and the number of lesions is usually less than 30.1,20 Lesions often appear in clusters (Figure 7) or in a linear pattern (eg, autoinoculated).11 Less commonly, the lesion can be solitary (Figure 8) at the time of presentation.21 The lesions are usually asymptomatic but may sometimes itch or become irritated.4,12 In congenital cases, the lesions may appear in a halo-like ring around the scalp.22 Rarely, a pale, hypopigmented ring or halo (Woronoff ring) around the lesion has been described (halo phenomenon).23

Figure 6.

Figure 7.

Figure 8.
At the point of regression, the lesion may appear inflamed characterized by swelling, erythema, crusting, and tenderness—a finding that signifies pending resolution of the lesion (Figure 9).6,14 The BOTE (beginning of the end) sign represents a host response that often precedes resolution of the disease rather than secondary bacterial superinfection.24 Likewise, an eczematous id reaction to the molluscum contagiosum virus may herald immunological clearance of the molluscum contagiosum lesion in an immunocompetent individual.25

Figure 9.
In immunocompromised individuals, the lesions can be very large and extensive (Figure 10).26 Also, the lesions may occur in atypical locations and may be atypical in appearance, such as verrucous and hypertrophic.4 The lesions tend to be rapidly progressive, disseminated, recalcitrant to treatment, and frequently recurring.27

Figure 10.
References
1. Badri T, Gandhi GR. Molluscum Contagiosum. In: StatPearls. StatPearls Publishing; March 21, 2021. http://www.ncbi.nlm.nih.gov/books/nbk441898/
2. Leung AK. Molluscum contagiosum. In: Leung AK, ed. Common Problems in Ambulatory Pediatrics: Specific Clinical Problems, Volume 1. Nova Science Publishers, Inc.; 2011;291-296.
3. Leung AK. The natural history of molluscum contagiosum in children. Lancet Infect Dis. 2015;15(2):136-137. https://doi.org/10.1016/s1473-3099(14)71061-8
4. Leung AKC, Barankin B, Hon KLE. Molluscum contagiosum: an update. Recent Pat Inflamm Allergy Drug Discov. 2017;11(1):22-31. https://doi.org/10.2174/1872213x11666170518114456
5. Forbat E, Al-Niaimi F, Ali FR. Molluscum contagiosum: review and update on management. Pediatr Dermatol. 2017;34(5):504-515. https://doi.org/10.1111/pde.13228
6. Moye V, Cathcart S, Burkhart CN, Morrell DS. Beetle juice: a guide for the use of cantharidin in the treatment of molluscum contagiosum. Dermatol Ther. 2013;26(6):445-451. https://doi.org/10.1111/dth.12105
7. Berbegal-DeGracia L, Betlloch-Mas I, DeLeon-Marrero FJ, Martinez-Miravete MT, Miralles-Botella J. Neonatal Molluscum contagiosum: five new cases and a literature review. Australas J Dermatol. 2015;56(2):e35-e38. https://doi.org/10.1111/ajd.12127
8. Olsen JR, Gallacher J, Piguet V, Francis NA. Epidemiology of molluscum contagiosum in children: a systematic review. Fam Pract. 2014;31(2):130-136. https://doi.org/10.1093/fampra/cmt075
9. Leung AK, Kong AY. Discrete papules on the thigh of a child. Molluscum contagiosum. Am Fam Physician. 2010;81(4):511. https://www.aafp.org/afp/2010/0215/p511.html
10. Schaffer JV, Berger EM. Molluscum contagiosum. JAMA Dermatol. 2016;152(9):1072. https://doi.org/10.1001/jamadermatol.2016.2367
11. Bard S, Shiman MI, Bellman B, Connelly EA. Treatment of facial molluscum contagiosum with trichloroacetic acid. Pediatr Dermatol. 2009;26(4):425-426. https://doi.org/10.1111/j.1525-1470.2009.00945.x
12. Meza-Romero R, Navarrete-Dechent C, Downey C. Molluscum contagiosum: an update and review of new perspectives in etiology, diagnosis, and treatment. Clin Cosmet Investig Dermatol. 2019;12:373-381. https://doi.org/10.2147/ccid.s187224
13. Ma H, Yang H, Zhou Y, Jiang L. Molluscum contagiosum on the lip. J Craniofac Surg. 2015;26(7):e681-e682. https://doi.org/10.1097/scs.0000000000002187
14. Fernando I, Pritchard J, Edwards SK, Grover D. UK national guideline for the management of genital molluscum in adults, 2014 Clinical Effectiveness Group, British Association for Sexual Health and HIV. Int J STD AIDS. 2015;26(10):687-695. https://doi.org/10.1177/0956462414554435
15. Demirdag HG, Ayanoglu BT, Durmus B, Bulut M, Akay BN. Molluscum contagiosum with dermoscopic features in an unusual areola and nipple location. Dermatol Online J. 2019;25(4):13030/qt0rz9q684. https://escholarship.org/uc/item/0rz9q684
16. Ringeisen AL, Raven ML, Barney NP. Bulbar conjunctival molluscum contagiosum. Ophthalmology. 2016;123(2):294. https://doi.org/10.1016/j.ophtha.2015.11.022
17. Falzon K, Scotcher S, Parulekar M. Primary epibulbar molluscum contagiosum in an immunocompetent child. J Pediatr. 2015;167(4):936. https://doi.org/10.1016/j.jpeds.2015.06.071
18. Kim HK, Jang WS, Kim BJ, Kim MN. Rare manifestation of giant molluscum contagiosum on the scalp in old age. Ann Dermatol. 2013;25(1):109-110. https://doi.org/10.5021/ad.2013.25.1.109
19. Bahalı AG, Su O, Ozkaya DB, et al. Plantar molluscum contagiosum in an adult patient. J Am Podiatr Med Assoc. 2016;106(3):235-236. https://doi.org/10.7547/15-019
20. Brown J, Janniger CK, Schwartz RA, Silverberg NB. Childhood molluscum contagiosum. Int J Dermatol. 2006;45(2):93-99. https://doi.org/10.1111/j.1365-4632.2006.02737.x
21. Kumar P, Savant SS. Solitary molluscum contagiosum. Indian Pediatr. 2015;52(8):723. https://doi.org/10.1007/s13312-015-0708-9
22. Nguy Nguyen HP, Franz E, Stiegel KR, Hsu S, Tyring SK. Treatment of molluscum contagiosum in adult, pediatric, and immunodeficient populations. J Cutan Med Surg. 2014;18(5):299-306. https://doi.org/10.2310/7750.2013.13133
23. Zawar V, Goyal T, Doda D. Woronoff ring: a novel manifestation of molluscum contagiosum. Skinmed. 2016;14(5):349-352.
24. Sil A, Bhanja DB, Chandra A, Biswas SK. BOTE sign in molluscum contagiosum. BMJ Case Rep. 2020;13(9):e239142. https://doi.org/10.1136/bcr-2020-239142
25. Netchiporouk E, Cohen BA. Recognizing and managing eczematous id reactions to molluscum contagiosum virus in children. Pediatrics. 2012;129(4):e1072-e1075. https://doi.org/10.1542/peds.2011-1054
26. Pérez-Díaz CE, Botero-García CA, Rodríguez MC, et al. Giant molluscum contagiosum in an HIV positive patient. Int J Infect Dis. 2015;38:153-155. https://doi.org/10.1016/j.ijid.2015.07.021
27. Ajithkumar VT, Sasidharanpillai S, Muhammed K, et al. Disseminated molluscum contagiosum following chemotherapy: a therapeutic challenge. Indian J Dermatol Venereol Leprol. 2017;83(4):516. https://doi.org/10.4103/0378-6323.193619