
Peer Reviewed
Acute Flaccid Myelitis
AUTHORS:
Ana-Maria Nae, MD
Resident Physician, Department of Family Medicine, Atrium Health, Charlotte, North Carolina
Stefanie Reed, DO
Pediatric Hospitalist, Department of Pediatrics, Atrium Health Levine Children’s Hospital, Charlotte, North Carolina
CITATION:
Nae A-M, Reed S. Acute flaccid myelitis [published online January 2, 2020]. Consultant360.
A 2-year-old previously healthy, fully-immunized right-hand–dominant boy presented to a children’s emergency department with acute-onset fever and paralysis of his right upper extremity.
History. The patient had been in his normal state of health until approximately 6 days prior, when he had received a diagnosis of acute otitis media, for which he had been treated with oral cefdinir. His parents reported that his condition had shown improvement during this time and that his fever initially had resolved. However, over the past 24 hours, the fever had returned, and they noted that he was not reaching for objects with his right upper extremity. The episode also was associated with acute constipation and urinary hesitancy. The patient had no history of trauma, seizure activity, swelling, neck stiffness, pain, or new exposures.
Physical examination. The patient had active and passive movement of the right wrist and hand, but he had no spontaneous movement of the right biceps, deltoid, or triceps muscles. Reflexes were absent at the right biceps. Additionally, the patient had some mild in-toeing of his right foot. Aside from these focal areas, he had normal reflexes, sensation, and movement. No swelling or deformity was noted. The remainder of the physical examination findings were nonfocal and age-appropriate, and he was playful, without distress.
Diagnostic tests. Results of a complete blood cell count were unremarkable, and the creatine phosphokinase level was normal. Inflammatory markers were mildly elevated. Plain radiographs of the affected area were normal.
Magnetic resonance imaging (MRI) of the cervical spine and right brachial plexus showed abnormal T2-weighted hyperintensity, most prominent at the craniocervical junction (Figure 1). MRI of the thoracic and lumbar spine showed abnormalities of the cauda equina similar to the cervical spine findings (Figure 2). Brachial plexus MRI findings were normal.

Figure 1. Sagittal MRI at C5-6 showing an abnormal heterogeneous speckled appearance.
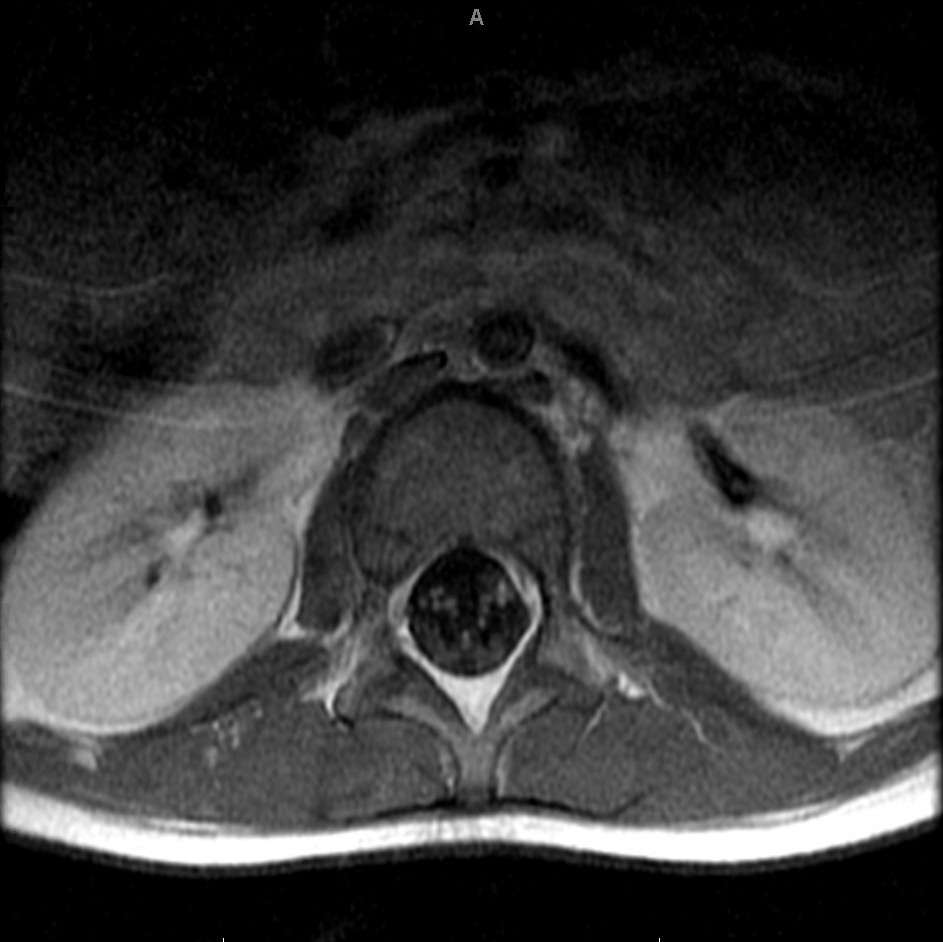
Figure 2. Axial MRI at the level of the conus showing abnormal heterogeneity in the spinal cord.
Cerebrospinal fluid (CSF) analysis showed isolated pleocytosis. Results of other CSF studies were unremarkable, including tests for West Nile virus, enterovirus, Epstein-Barr virus, and aquaporin-4 antibodies, as well as a fluid culture. A respiratory pathogen panel was not obtained given the lack of clear respiratory tract symptoms in this patient; however, results of fecal enterovirus polymerase chain reaction results were ultimately positive.
Discussion. Acute flaccid myelitis (AFM) is a rare syndrome characterized by flaccid weakness in one or more limbs with distinct abnormalities of the spinal cord gray matter seen on MRI.1 Since 2014, there has been a significant increase in the number of reports of AFM in the United States, with nonpolio enteroviruses commonly being implicated. Per Centers for Disease Control and Prevention (CDC) guidelines, reportable cases include any person with an acute onset of flaccid limb weakness, and either MRI findings of a spinal cord lesion largely restricted to the gray matter, spanning one or more vertebral segments, or CSF showing pleocytosis.1
AFM is considered a subtype of acute flaccid paralysis (AFP), which also includes Guillain-Barré syndrome and acute transverse myelitis. AFM is most commonly attributable to infection with poliovirus or flaviviruses such as West Nile virus. However, a growing number of other viruses, including nonpolio enteroviruses, are being reported to the CDC in association with AFM each year.
The discussion of enteroviruses includes polioviruses, echoviruses, and coxsackieviruses, which all tend to display seasonal variation.2,3 For example, in the summer and fall of 2014, the United States and Canada experienced epidemic numbers of enterovirus D68 (EV-D68) infections (Figures 3 and 4).4,5 These cases predominantly presented with severe respiratory manifestations. Reports of AFP with positive EV-D68 findings rose during this period, leading investigators to suggest a clear association between the two.6,7 With this upsurge in reported AFM cases, the CDC began standardized surveillance in 2015.1,8
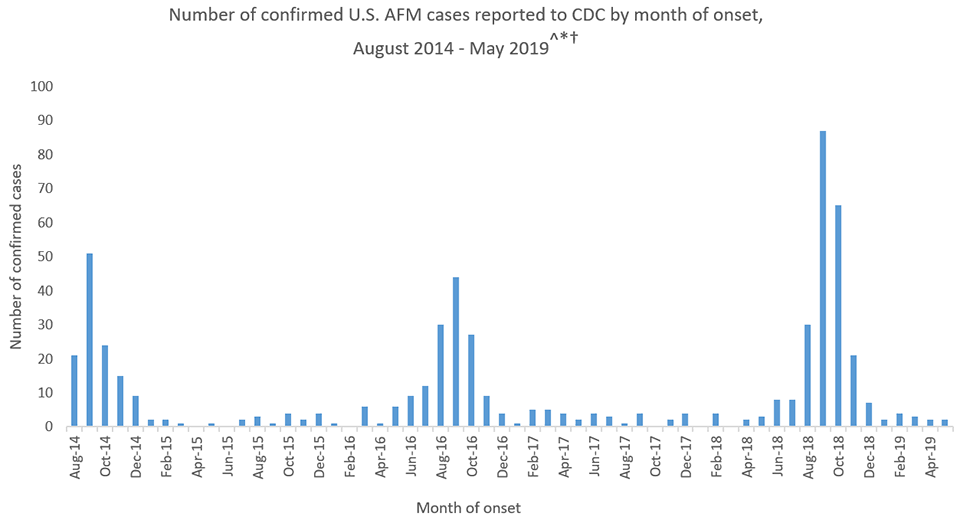
Figure 3.4
Resolution outcomes in these patients are mixed, as are results of treatment trials. Most patients to date have been treated with intravenous immunoglobulin (IVIG) 2g/kg administered once, pulse-dose corticosteroids, or a combination of both. Despite these interventions, most treated patients continue to have motor deficits at follow-up.5,7 Thus, the CDC does not endorse enteroviral-associated AFM as a clear indication for either intervention.8 The risks and benefits of each treatment should be discussed and weighed between each family and medical team.
AFM from nonpolio enterovirus continues to represent a small but important minority of AFM case reports submitted to the CDC. As of November 26, 2019, there were 32 confirmed cases in the United States; In 2018 there were 237 confirmed cases in 41 states (Figure 4).4 More than 90% of all cases involve children, most commonly in those with a preceding respiratory or febrile illness.8 While AFM remains a diagnosis of exclusion, it should be considered in any patient meeting simple diagnostic criteria, particularly during peak seasons (August through October). Parents and patients should be counseled on the long-term prognosis and lack of standardized treatment protocols for this illness. This diagnosis is ultimately a multidisciplinary team case.
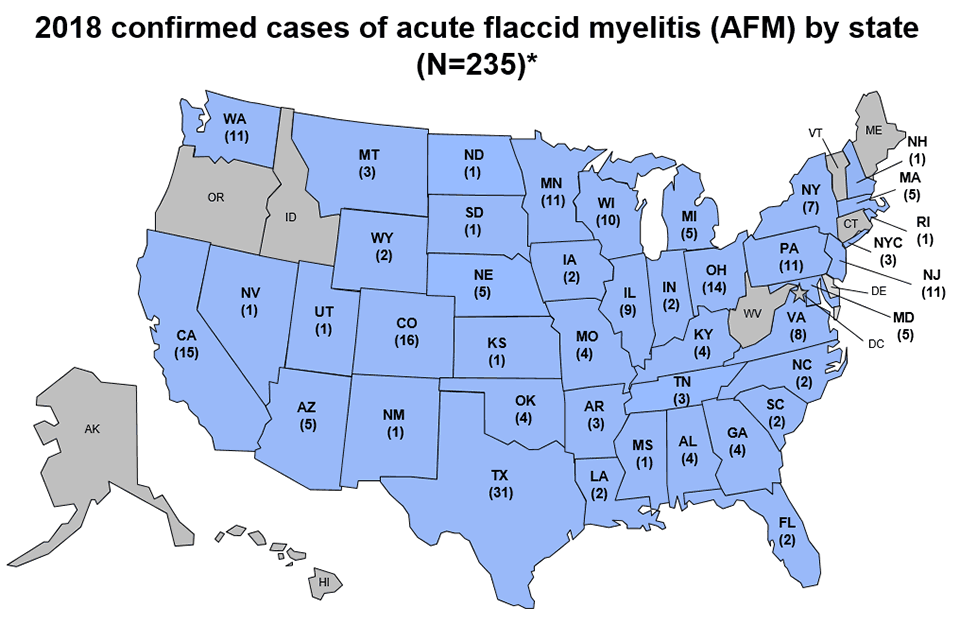
Figure 4.4
Outcome of the case. This patient’s case was confirmed as AFM by the CDC shortly after testing. After consultation with the pediatric neurology team at our institution, he was empirically started on a 5-day course of intravenous methylprednisolone. His multidisciplinary team offered IVIG therapy, but the parents ultimately decided to forego this treatment option after discussion of the indeterminate prognosis and the IVIG infusion risk profile.
At time of discharge, the boy continued to exhibit right extremity paralysis to the elbow, as well as decreased biceps deep tendon reflex. However, at a 3-month follow-up visit, he had a slight return of some elbow flexion. Repeated MRI of the cervical, thoracic, and lumbar spine showed interval resolution of the previous abnormal spinal cord signal changes. He continues with outpatient physical and occupational therapies, and he has been evaluated for nerve transplant candidacy at a specialty center outside of our system.
REFERENCES:
- DeBolt C. Revision to the Standardized Surveillance and Case Definition for Acute Flaccid Myelitis [position statement]. Atlanta, GA: Council of State and Territorial Epidemiologists; 2017. 17-ID-0 https://cdn.ymaws.com/www.cste.org/resource/resmgr/2017PS/2017PSFinal/17-ID-0pdf. Accessed December 17, 2019.
- American Academy of Pediatrics. Enterovirus (nonpoliovirus) (group A and B coxsackieviruses, echoviruses, numbered enteroviruses). In: Kimberlin DW, Brady MT, Jackson MA, eds. Red Book: 2018-2021 Report of the Committee on Infectious Diseases. 31st ed. Itasca, IL: American Academy of Pediatrics; 2018:331-334.
- Centers for Disease Control and Prevention. Non-polio enterovirus. https://www.cdc.gov/non-polio-enterovirus/index.html. Reviewed November 14, 2018. Accessed December 17, 2019.
- Centers for Disease Control and Prevention. AFM Cases in U.S. https://www.cdc.gov/acute-flaccid-myelitis/cases-in-us.html. Reviewed December 3, 2019. Accessed December 17, 2019.
- Nelson GR, Bonkowsky JL, Doll E, et al. Recognition and Management of Acute Flaccid Myelitis in Children. Pediatr Neurol. 2016;55:17-21. doi:10.1016/j.pediatrneurol.20110.007
- Greninger AL, Naccache SN, Messacar K, et al. A novel outbreak enterovirus D68 strain associated with acute flaccid myelitis cases in the USA (2012-14): a retrospective cohort study. Lancet Infect Dis. 2015;15(6):671-682. doi:10.1016/S1473-3099(15)70093-9
- Yoder JA, Lloyd M, Zabrocki L, Auten J. Pediatric acute flaccid paralysis: enterovirus D68-associated anterior myelitis. J Emerg Med. 2017;53(1):e19-e23. doi:10.1016/j.jemermed.20103.020
- Centers for Disease Control and Prevention. AFM investigation. https://www.cdc.gov/acute-flaccid-myelitis/afm-investigation.html. Reviewed November 4, 2019. Accessed December 17, 2019.