
Peer Reviewed
Focal Acral Hyperkeratosis in an Adolescent
AUTHORS:
Ciara Grayson, MS1 • Candrice R. Heath, MD2
AFFILIATIONS:
1 Florida State University College of Medicine, Tallahassee, Florida
2 Lewis Katz School of Medicine, Temple University, Philadelphia, Pennsylvania
CITATION:
Grayson C, Heath CR. Focal acral hyperkeratosis in an adolescent. Consultant. 2021;61(10):e24-e26. doi:10.25270/con.2021.02.00003
Received August 7, 2020. Accepted December 9, 2020. Published online February 8, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Ciara Grayson, MS, Florida State University College of Medicine, 1115 West Call Street, Tallahassee, Florida 32304 (ciaragrayson5@gmail.com)
A 16-year-old girl presented to our dermatology clinic with a rash on her feet, which had been present for 10 years. The asymptomatic rash had started on her right foot but progressed to the left foot over the past 3 to 6 months.
History. Her medical history was significant for eczema as a child. She had had no developmental disorders during childhood. Four years prior to presentation, the patient had taken griseofulvin for a few months without improvement. She had used products containing lactic acid, urea, and salicylic acid in the past, but they were not successful in treating the rash.
Physical examination. The physical examination at that time revealed polygonal, keratotic papules, many of which had slightly depressed centers on the marginal border of bilateral feet (Figure 1).

After a 4-month trial of over-the-counter lactic acid, the patient returned for a follow-up visit. The findings of the physical examination of her feet at the follow-up visit were unchanged since her initial presentation, but new, barely perceptible, similar round and polygonal papules were noted on the marginal border of her hands.
Laboratory tests. A skin biopsy of the right lateral plantar foot showed compact orthokeratosis overlying regular epidermal hyperplasia with mildly thickened collagen in the dermal papillae (Figure 2). The histological findings confirmed the diagnosis of focal acral hyperkeratosis.

Discussion. Focal acral hyperkeratosis was first described in 1983 as a condition that is clinically identical to acrokeratoelastoidosis, but it lacks elastorrhexis on histological examination.1 Acrokeratoelastoidosis was first described in 1953 as a skin eruption with small, waxy, translucent papules that gradually appear on the margins of an individual’s hands or feet over the years.2,3 These papules frequently come together to form plaques.
Although very similar, histological examination can differentiate these 2 conditions. Focal acral hyperkeratosis is more common in Black women.1,4 Familial cases of focal acral hyperkeratosis have been reported, in which the mode of inheritance appears to be autosomal dominant. In our case, the mother of our patient self-reported having a “foot rash” that resolved, but the diagnosis of the rash was uncertain and likely unrelated to this case.
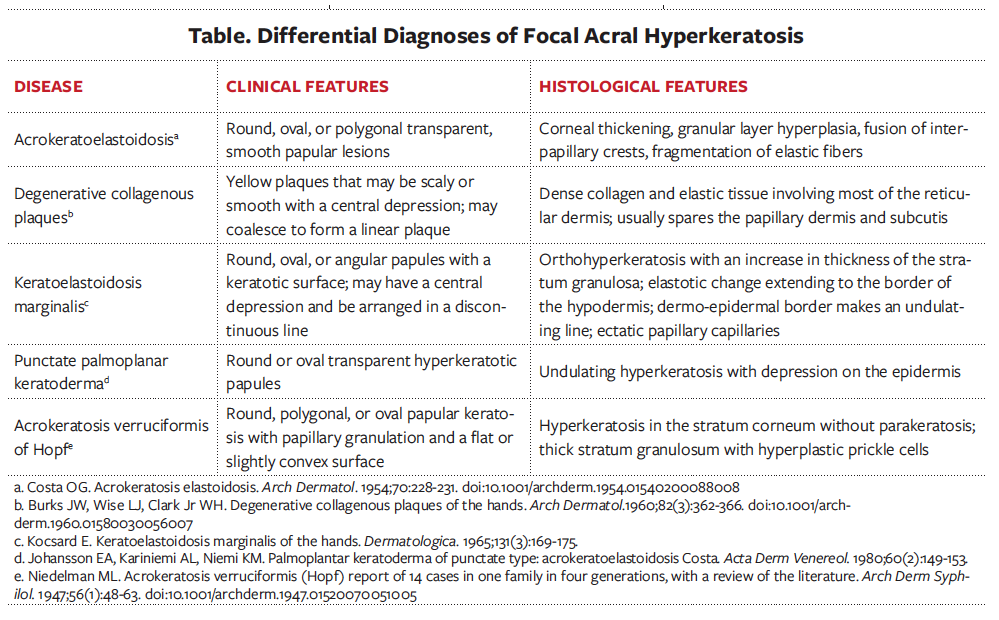
Sporadic cases of focal acral hyperkeratosis have also reported.1 The main differential diagnoses of focal acral hyperplasia include acrokeratoelastoidosis, keratoelastoidosis marginalis, degenerative collagenous plaques, punctate palmoplanar keratoderma, and acrokeratosis verruciformis. They can be differentiated by clinical and histological features (Table).
Treatment. Treatment options that have proved to be unsuccessful for acrokeratoelastoidosis and focal acral hyperkeratosis include liquid nitrogen, salicylic acid, tretinoin, and prednisone.3 In one case, a 14-year-old boy with a 12-year history of acrokeratoelastoidosis used tretinoin, 0.1%, topical cream twice daily for approximately 1 year, but he did not show any improvement.3
In a case of a 25-year-old Black woman, treatment with topical calcipotriol twice daily for 8 weeks led to significant improvement.5 There was no recurrence of focal acral hyperkeratosis 8 months after treatment.5
In another report, a 9-year-old girl with lesions for 8 years was treated with salicylic acid, 3%, and tretinoin, 0.1%, but she had no response in 3 months.6 Another case reported improvement in 1 month after using etretinate, 50 mg, daily.7 In 6 months, there was marked flattening of the papules. However, when etretinate was reduced to 25 mg daily, the lesions worsened. When etretinate was stopped completely, the papules recurred but were less prominent than before starting treatment.7 Additionally, treatment with the erbium:YAG laser resulted in flattening of a patient’s papules, and no recurrence was seen after 6 months.8 There are no cases of spontaneous resolution of focal acral hyperkeratosis in the literature published in English.
Outcome of the case. Our patient tried a short course of an over-the-counter lotion containing lactic acid for 2 weeks, which did not affect the lesions. Due to the brevity of treatment, it is difficult to document this as a treatment failure. The condition bothered the mother more than the patient, which provides some insight into motivation for adherence for this patient.
- Dowd PM, Harman RRM, Black MM. Focal acral hyperkeratosis. Br J Dermatol. 1983;109(1):97-103. doi:10.1111/j.1365-2133.1983.tb03997.x
- Costa OG. Acrokeratosis elastoidosis. Arch Dermatol. 1954;70:228-231. doi:10.1001/archderm.1954.01540200088008
- Nelson-Adesokan P, Mallory SB, Leonardi CL, Lund R. Acrokeratoelastoidosis of Costa. Int J Dermatol. 1995;34(6):431-433. doi:10.1111/j.1365-4362.1995.tb04448.x
- Blum SL, Cruz Jr PD, Siegel DM, Tigelaar RE. Hyperkeratotic papules on the hands and feet. Focal acral hyperkeratosis (FAH). Arch Dermatol. 1987;123(9):1225-1226. doi:10.1001/archderm.123.9.1225a
- Ballambat SP, Pai K. Acquired crateriform hyperkeratotic papules of the feet: an unusual variant of focal acral hyperkeratosis. Indian J Dermatol Venereol Leprol. 2007;73(5):359-361. doi:10.4103/0378-6323.35749
- Erkek E, Koçak M, Bozdoğan O, Atasoy P, Birol A. Focal acral hyperkeratosis: a rare cutaneous disorder within the spectrum of Costa acrokeratoelastoidosis. Pediatr Dermatol. 2004;21(2):128-130. doi:10.1111/j.0736-8046.2004.21208.x
- Handfield-Jones S, Kennedy CT. Acrokeratoelastoidosis treated with etretinate. J Am Acad Dermatol. 1987;17(5 Pt 2):881-882. doi:10.1016/s0190-9622(87)70273-4
- Erbil AH, Sezer E, Koç E, Tunca M, Tastan HB, Demiriz M. Acrokeratoelastoidosis treated with the erbium:YAG laser. Clin Exp Dermatol. 2008;33(1):30-31. doi:10.1111/j.1365-2230.2007.02553.x