
Peer Reviewed
Terson Syndrome: A Case of Intraocular Hemorrhage Secondary to Intracerebral Hemorrhage
AUTHORS:
Kenneth Lam, MD1 • Nisarg Joshi, MD2 • Jonathan Tsui, MD2 • Benjamin Hale, MD2
AFFILIATIONS:
1Geisinger Commonwealth School of Medicine, Scranton, Pennsylvania
2Geisinger Eye Institute, Geisinger Medical Center, Danville, Pennsylvania
CITATION:
Lam K, Joshi N, Tsui J, Hale B. Terson syndrome: a case of intraocular hemorrhage secondary to intracerebral hemorrhage. Consultant. 2022;62(6);e17-e19. doi:10.25270/con.2021.11.00001
Received May 14, 2021. Accepted June 22, 2021. Published online November 8, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Kenneth Lam, MD, Geisinger Commonwealth School of Medicine, 525 Pine Street, Scranton, PA 18510 (klam@som.geisinger.edu)
A 61-year-old man presented to our neuro-ophthalmology department for evaluation of vision loss following a recent hospital discharge.
History. He had been admitted to the hospital for a subdural hematoma secondary to a fall and required hemicraniectomy with clipping and resection of 2 distal right middle cerebral artery aneurysms. The patient's clinical course had been complicated by recent endocarditis and a mitral valve abscess, which had been treated with ceftriaxone therapy. Upon extubation, the patient had reported bilateral blurry vision.
One month after the injury, the patient presented to our ophthalmology clinic. At that time, he had a visual acuity of 20/300 in the right eye and 20/150 in the left eye. Fundoscopic examination and imaging showed multifocal areas of preretinal and intraretinal hemorrhage in multiple layers of the retina in the posterior pole (Figure 1). Ocular coherence tomography imaging of the macula helped characterize the bilateral subinternal-limiting membrane hemorrhages, bilateral outer retinal irregularity, and pigment migration in the right fovea (Figures 2 and 3).
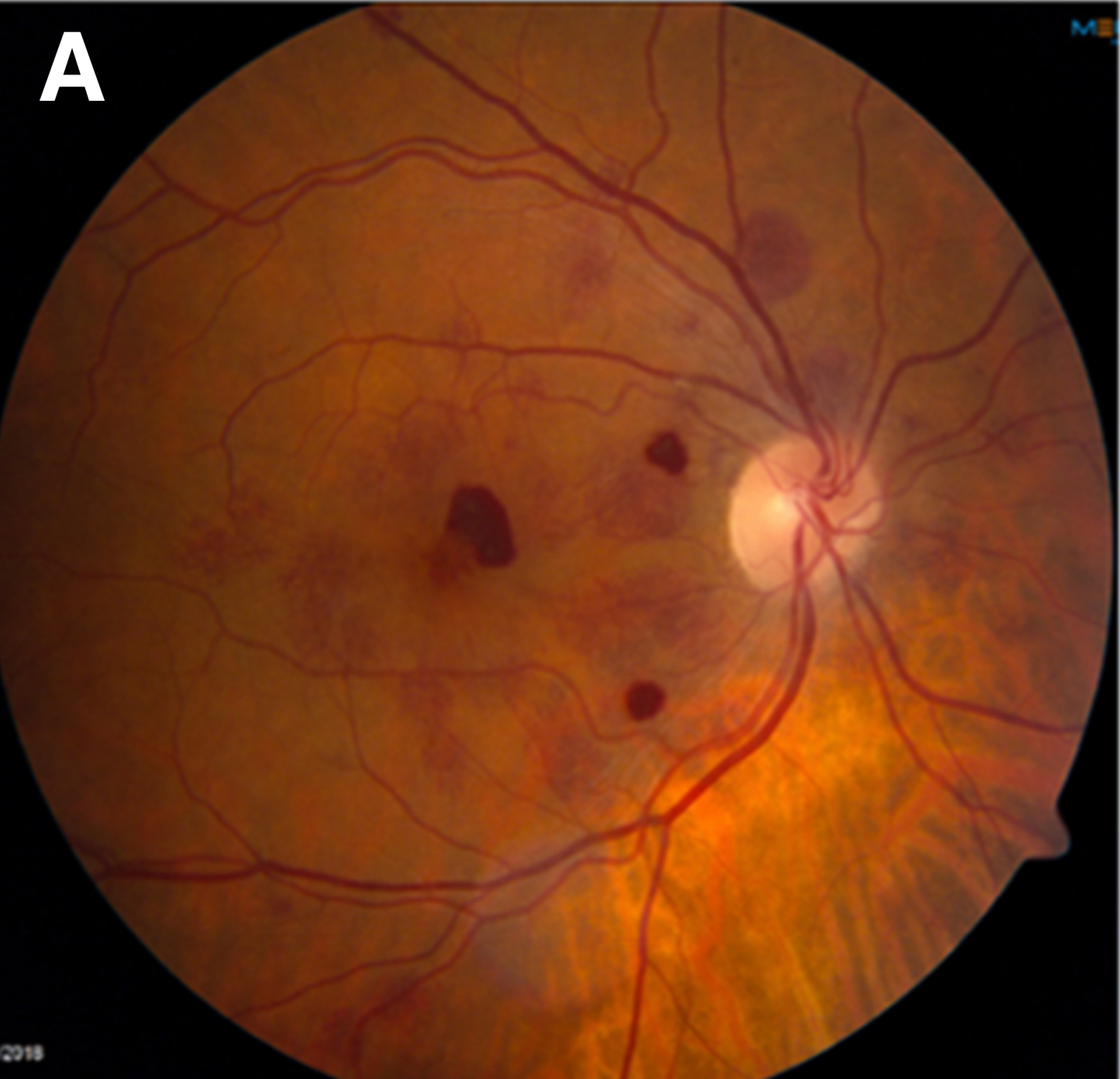



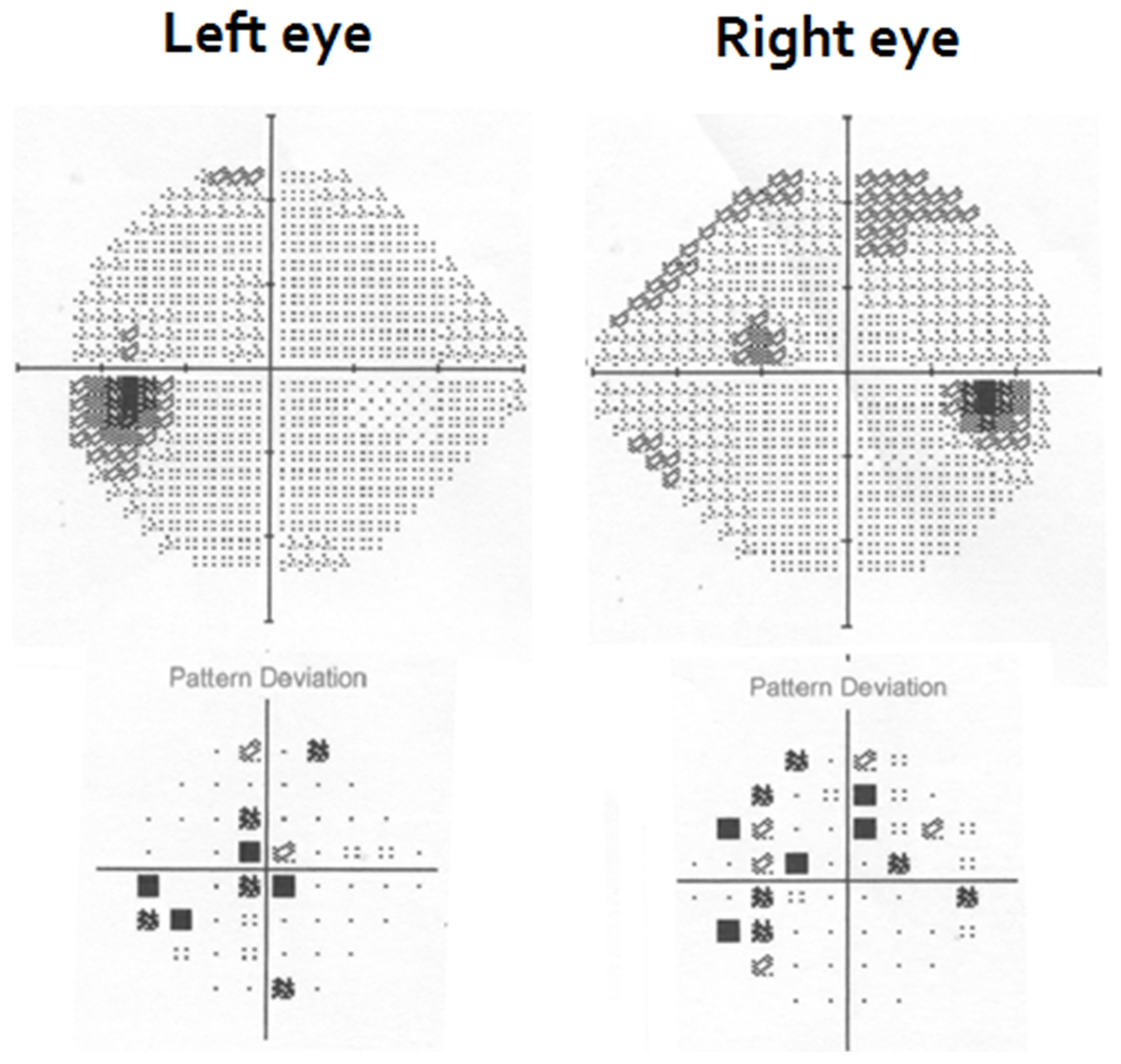
While Roth spots were considered in the differential diagnosis given the patient’s endocarditis, the distribution, size, and level of hemorrhages were inconsistent with infectious emboli. Instead, the hemorrhages were thought to be related to the intracranial hemorrhage and subsequent hemicraniectomy with aneurysm clippings and resections. Visual field testing showed patchy deficits bilaterally, which corresponded to preretinal and intraretinal hemorrhages found on fundoscopic examination and imaging (Figure 4). The visual field deficits were not consistent with damage to the visual pathway or the occipital lobe. Therefore, the patient received a diagnosis of Terson syndrome.
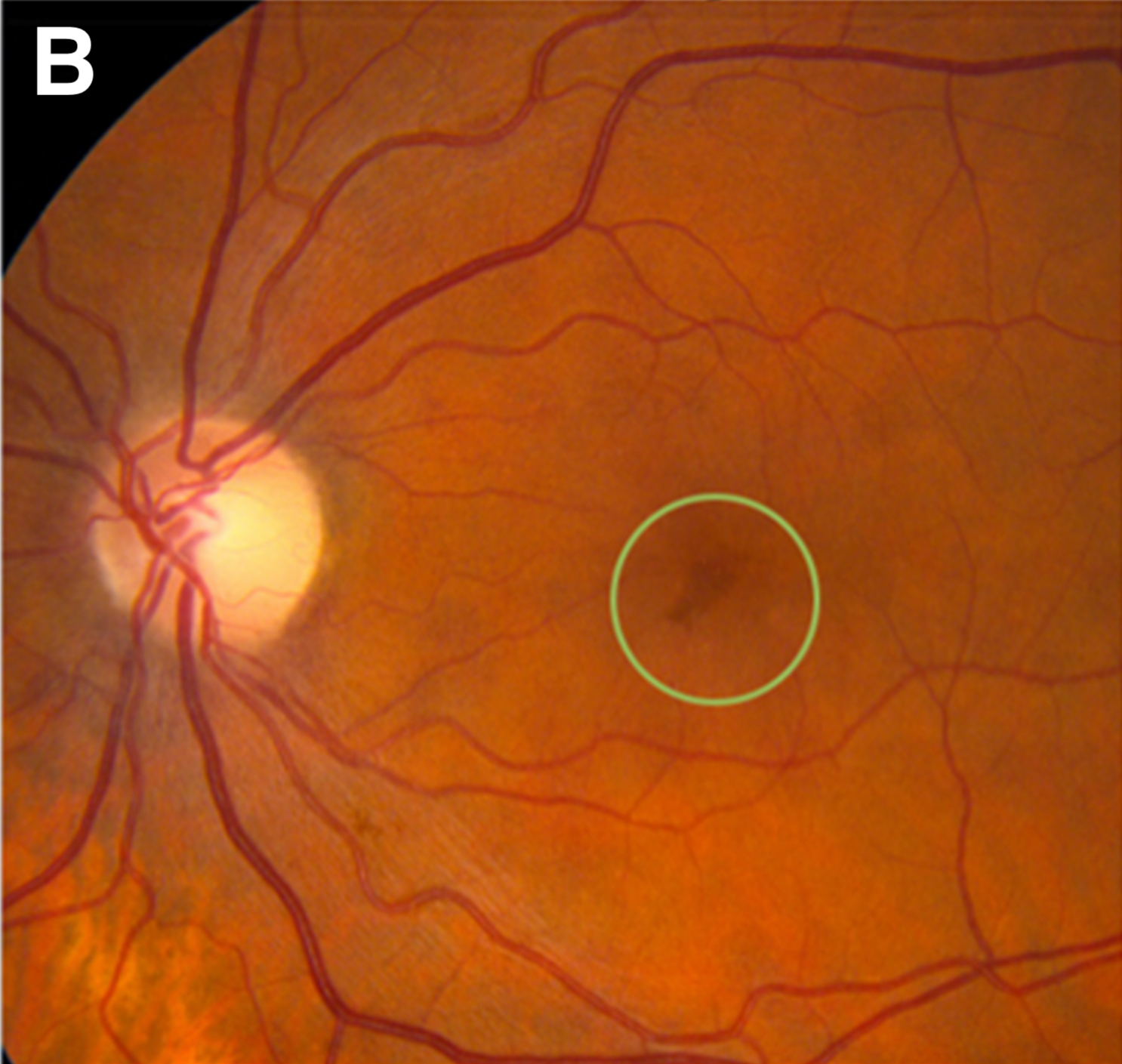
Over the course of 7 months, the patient’s intraretinal hemorrhages spontaneously resolved. At 4 months post-injury, bilateral fundoscopic photos revealed near-complete resolution of retinal hemorrhages (Figure 5). Ocular coherence tomography imaging at 7 months of both maculae showed resolution of hemorrhages and with subtle damage to the outer retina, likely from blood toxicity (Figures 2 and 3).

The patient regained a significant amount of vision (20/30 in the right eye; 20/40 in the left eye) and did not show loss of neurologic function at 8 months post-injury.
Discussion. Terson syndrome is an uncommon intraocular hemorrhage (ie, vitreous, subhyaloid, subretinal space, or beneath the internal limiting membrane) classically associated with subarachnoid hemorrhage but can also be associated with intracerebral hemorrhage and traumatic brain injury.1 Terson syndrome symptoms can vary depending on the location and severity of intraocular hemorrhage but usually manifest as floaters, partial vision loss, or total vision loss.2 While patients with an acute onset of decreased visual acuity should promptly receive an ophthalmic examination, patients with subarachnoid hemorrhage, intracerebral hemorrhage, or traumatic brain injury may be unable to communicate ocular deficits because of neurological impairment, and delays in diagnosis and treatment may lead to permanent vision loss. Physicians managing patients with aneurysmal bleeds should be cognizant of the association with Terson syndrome and obtain an ophthalmic evaluation.
Terson syndrome is the finding of retinal hemorrhages in multiple layers of the eye that are classically associated with subarachnoid or other intracerebral hemorrhage and traumatic brain injury. The etiology of Terson syndrome is still not fully understood, but it is thought that an acute increase in intracranial pressure acts on the optic sheath, causing compression of the venous outflow at the level of the central retinal vein leading to venous hypertension and rupture of retinal capillaries.3 Previously accepted theories suggest that intraocular hemorrhages may be an extension of subarachnoid blood through the optic sheath. The resulting intraocular hemorrhage can lead to irreversible damage to the retina through ischemia or toxicity to the retinal photoreceptors.
Although the symptoms of Terson syndrome can vary from asymptomatic to sudden total loss of vision, the ophthalmic prognosis is favorable since symptoms affecting vision loss are usually reversible with spontaneous resolution of the intraocular hypertension over time. In patients with vitreous hemorrhage that does not resolve in a timely manner, vitrectomy can improve vision. Unlike the ophthalmic prognosis, however, survival outcomes in patients with subarachnoid hemorrhage and intraocular hypertension carry a poor prognosis with increased mortality compared with patients without intraocular hypertension (50% vs 9%).4 The decrease in survival rate among patients with Terson syndrome can be attributed to the increased severity of the subarachnoid hemorrhage, as the median Hunt and Hess Scale, Glasgow Coma Scale, and Fisher Grading Scale for Subarachnoid Hemorrhage are typically significantly worse compared with patients with subarachnoid hemorrhage without Terson syndrome.5
Patient outcome. Terson syndrome is classically associated with subarachnoid hemorrhage, but our patient presented with a subdural hematoma. During the early course of his subdural hematoma, it is suspected that an acute change in his intracranial pressure caused intraocular vessels to rupture and that his intraretinal hemorrhages occurred without direct ocular trauma or involvement. Additionally, our patient did not develop a vitreous hemorrhage and did not require a vitrectomy. Although an intracerebral bleed plus intraocular hypertension is associated with a poor prognosis and high mortality rate, our patient showed no loss of neurologic function and regained a significant amount of vision.
Conclusions. While a timely ophthalmic evaluation should be performed on any patient with an acute decrease in visual acuity, special consideration should be taken with patients with subarachnoid hemorrhage, intracerebral hemorrhage, or traumatic brain injury, as they may have neurological impairments that prevent them from communicating their ocular deficits.
1. Czorlich P, Skevas C, Knospe V, et al. Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury. Neurosurg Rev. 2015;38(1):129-136. https://doi.org/10.1007/s10143-014-0564-4
2. Mazurek M, Krzystolik K, Lachowicz E, Kubasik-Kladna K, Czepita D. Terson syndrome--a literature review. Klin Oczna. 2014;116(1):59-63.
3. Gress DR, Wintermark M, Gean AD. A case of Terson syndrome and its mechanism of bleeding. J Neuroradiol. 2013;40(4):312-314. https://doi.org/10.1016/j.neurad.2013.07.003
4. Sung W, Arnaldo B, Sergio C, Juliana S, Michel F. Terson's syndrome as a prognostic factor for mortality of spontaneous subarachnoid haemorrhage. Acta Ophthalmol. 2011;89(6):544-547. https://doi.org/10.1111/j.1755-3768.2009.01735.x
5. Czorlich P, Skevas C, Knospe V, Vettorazzi E, Westphal M, Regelsberger J. Terson's syndrome - Pathophysiologic considerations of an underestimated concomitant disease in aneurysmal subarachnoid hemorrhage. J Clin Neurosci. 2016;33:182-186. https://doi.org/10.1016/j.jocn.2016.04.01